Caught in a Spiral: The crash of Airwork flight 23

On the 3rd of May 2005, residents of a rural area of New Zealand’s North Island, hearing the roar of engines, followed by an explosion, looked up into the night sky to see a fireball descending. They bore witness to the final seconds of Airwork flight 23, a routine New Zealand mail flight which had abruptly spiraled out of control and disintegrated in the air, killing both pilots and leaving debris strewn across a wide area of forest and pastureland. What could have caused the twin-engine Fairchild Metroliner to come apart so catastrophically? Only the black boxes held the answers, locked away in the final conversations of the deceased flight crew. What investigators discovered therein was a surprising and unique sequence of events, beginning with an ill-advised attempt to transfer fuel between the tanks, and ending with a spiral dive that ripped the plane apart in midair.
◊◊◊

One of New Zealand’s oldest aviation companies is Airwork, which has operated continuously for 86 years — but most Kiwis have probably never heard of it. That’s because Airwork isn’t an airline, but a company which leases its aircraft and crews to other airlines, for purposes ranging from cargo and passenger charters to mail runs to various government functions. Airwork planes have operated for numerous airlines in Oceania and beyond, including Virgin Australia, Parcelair, and Toll Priority, and usually appear in these companies’ liveries rather than their own. That has rendered Airwork largely invisible, despite its modern fleet of nearly two dozen Boeing jets and almost 30 helicopters.

In the past, Airwork has also operated a number of smaller aircraft, including the Fairchild-Swearingen SA227 Metro III, a 19-passenger twin-engine turboprop popularly known as the Metroliner. The model’s large number of names has to do with its complicated development history, which began at Swearingen Aircraft in the 1960s before being taken over by Fairchild in the early 1970s. The Metroliner was an odd-looking aircraft with a long, pointy nose, a narrow, cramped cabin, and diminutive landing gear which stowed forward instead of backward or inward . Pilots had a love-hate relationship with the plane, although the nicknames they gave it suggested that there was more hate than love, as it was derisively known as the “Texas Lawn Dart,” “San Antonio Sewer Pipe,” “Screamin’ Weenie,” “Terror Tube,” “Widowmaker,” “Kerosene Crowbar,” “Necroliner,” and about a dozen other similar names, some of them obscene.

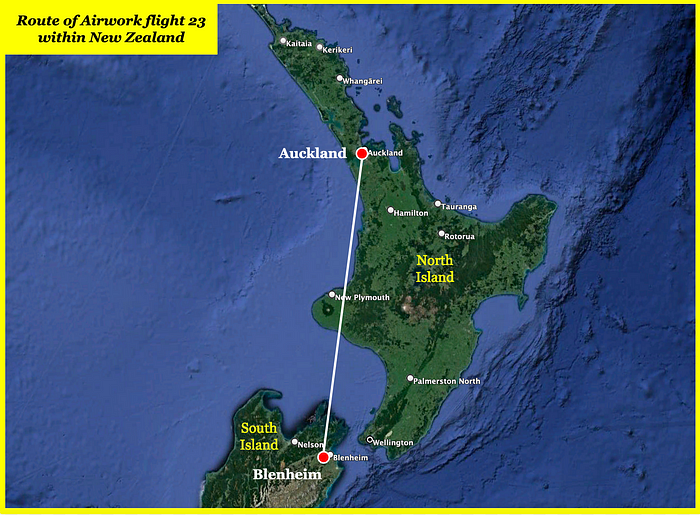
It was just such a Metroliner, configured to carry cargo instead of passengers, which was scheduled to perform a routine contract mail-carrying flight on the 3rd of May 2005 from Auckland, New Zealand’s largest city, to Woodbourne Airport near Blenheim, on the northern tip of South Island. In command of the flight, known by its callsign “Post 23,” was 43-year-old Captain Clive Adamson, a relatively experienced pilot and line check captain with 6,500 total hours, nearly half of them on the Metroliner. Joining him was a much less experienced first officer, 41-year-old Anthony Drummond, who had 2,300 flying hours but only 70 on the Metroliner, which he had started flying earlier that year. No one else was on board, nor was there room, since the entire cabin was full of palletized mail.
It was the mail itself which set in motion the bizarre and unexpected sequence of events which followed. Complications during the loading process led to a delay which put flight 23 fifteen minutes behind schedule by the time the pilots summoned the fuel truck shortly before engine start. On the Metroliner, it was standard procedure to split the fuel evenly between the right and left wing tanks, ensuring a proper balance. But this process required disconnecting, moving, and then reconnecting the fuel truck, which took time, so the pilots decided to save a couple of minutes by directing the refueling operator to put all the fuel into the left wing tank only.
After taking on 1,000 pounds (450 kg) of fuel, the pilots sought to balance the load prior to takeoff by using the Metroliner’s unusual gravity-driven crossflow system.
Most transport aircraft allow transfer of fuel between the tanks using a pump-driven cross-feed system, but the Metroliner and related models are unique in that they lack cross-feed pumps. Instead, the Metroliner has a crossflow system which runs between the bottom of each tank, causing gravity to equalize the fuel levels, as the fuel’s own weight pushes it through the crossflow line and up into the other tank until the two tanks achieve equilibrium.
While there is no formal procedure for doing so, this process can be expedited in a number of different ways. While on the ground, one way to do this is to make repeated tight turns with the target tank on the outside of the turn, forcing fuel through the crossflow line faster. Although this looks rather silly, it is effective, and so the pilots of flight 23 requested permission from Auckland ground control to essentially do some donuts on the apron while taxiing to the runway.
Although the flight data recorder revealed that the crew did indeed make at least one tight 360-degree turn prior to lining up for takeoff, it is not known for sure how much fuel this would have transferred. During the ten minutes between engine start and takeoff, the crossflow system should normally be able to transfer 500 pounds (225 kg) of fuel. Nevertheless, it remains unknown whether flight 23 was in compliance with the company’s fuel imbalance limit of 200 pounds (90kg) when it took off at 21:15.
With First Officer Drummond at the controls, flight 23 climbed toward its cruising altitude of 18,000 feet with the autopilot engaged. However, turbulence at that altitude was heavy, so Captain Adamson requested and received permission to climb to 22,000 feet to get above it. No mention was made of the fact that use of the Metroliner’s autopilot was prohibited above 20,000 feet.
The Metroliner and related aircraft were not originally manufactured with an autopilot, but three of Airwork’s six Metroliners, including this one, had autopilots installed as an aftermarket feature. Test flights by autopilot manufacturer Rockwell Collins had shown that the system could not maintain an acceptable margin above the stall speed at high altitudes, especially while maneuvering, so the Metroliner flight manual was amended to include a limitation on the altitudes at which the autopilot could be used. The pilots of flight 23, however, must not have been aware of this rule, because they leveled off at 22,000 feet with the autopilot still engaged.
For fifteen minutes after leveling off, the pilots kept the engines at climb power to increase their speed and make up for lost time, but otherwise all seemed normal. Some light ice buildup occurred, which was easily reversed by the plane’s de-icing systems. The aircraft soon emerged from the clouds, and the pilots commented on the starry sky above them. Someone reduced engine power from climb back to cruise.
Then, at 22:12, Captain Adamson must have decided that there was still an unacceptable imbalance between the plane’s two fuel tanks, because he said, “We’ll just open the crossflow again… sit on the left ball and trim it accordingly.”
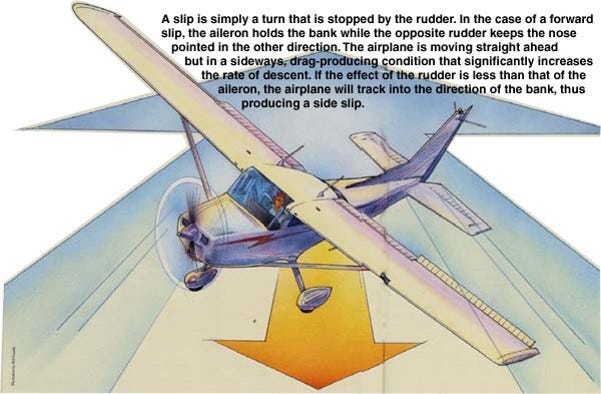
Adamson’s intention was to employ a procedure intended to expedite fuel transfer while in the air. It was obviously impossible to throw the fuel from one tank to the other by doing donuts, but in flight the process could be sped up using a gravity assist. Although there was no written procedure for doing so, Airwork had been teaching its pilots to increase fuel transfer through the crossflow line by banking the wings slightly in the direction of the target fuel tank, causing the fuel to flow downhill. This would also cause the plane to turn in that direction, so to keep it flying straight, the pilot needed to turn the opposite way using the rudder. In this case, since the right wing tank was the target, this meant that the pilots intended to bank slightly right, then use the rudder to point the nose slightly left, putting the plane into a crab-like right sideslip. (The direction of sideslip is based on which side of the plane points into the wind, not where the nose is pointing.)
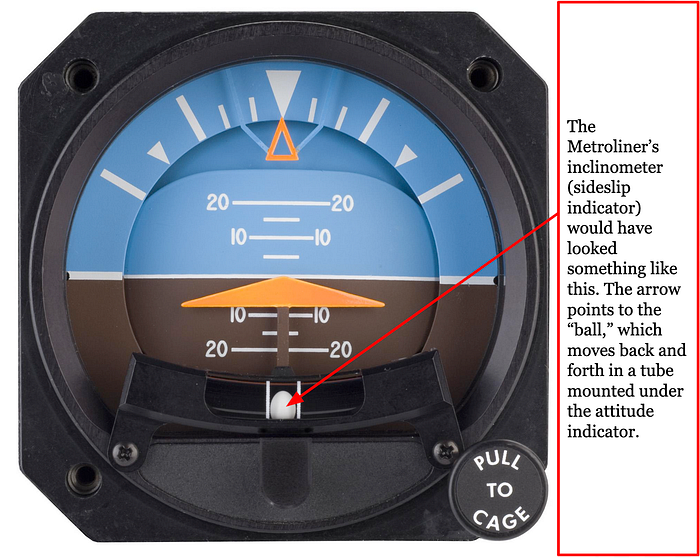
On the Metroliner, the amount of sideslip could be measured using an inclinometer, an instrument which consisted of a ball inside a liquid-filled glass tube. If the nose was pointing in a direction other than the direction of travel — in other words, if the plane was in a sideslip — the ball would move toward the direction of the sideslip. So when Captain Adamson said “sit on the left ball,” he meant “turn left with the rudder to move the ball in the inclinometer.”
The next step, after achieving such a sideslip, was to preserve it using the rudder trim system. The rudder trim is used to bias the rudder in a particular direction, allowing a continuous input to be made without the pilot having to apply force to the rudder pedals. When Captain Adamson said “trim it accordingly,” he meant for First Officer Drummond to apply left rudder trim until he no longer needed to touch the rudder pedals to maintain the sideslip.
In response, Drummond opened the crossflow valve and began to push on the rudder to achieve a right sideslip. Over the next 19 seconds, Adamson repeated his instructions several more times, telling Drummond to “Step on the left pedal, and just trim it to take the pressure off,” and “Get the ball out to the right as far as you can.” He seemed to be under the impression that the maneuver required a large sideslip angle, even though a small one would have sufficed.
First Officer Drummond, clearly uncomfortable inducing such a large sideslip in cruise flight, said “I was being a bit cautious,” and asked Adamson whether he was sure about the procedure.
“Don’t be cautious mate, it’ll do it good,” Adamson replied.
Encouraged by his captain’s instructions, First Officer Drummond pushed the plane into a large sideslip. The autopilot immediately compensated, holding the plane on course by banking to the right. Drummond then added left rudder trim until the plane stabilized in the sideslip and he could let go of the pedals. “How’s that?” he asked.
“That’s good — should come right — hopefully it’s coming right,” said Adamson, referring to the fuel, which was now flowing downhill into the right wing tank.
The pilots of flight 23 had now put their airplane into a delicate dance at 22,000 feet. With the rudder trimmed almost full left, the plane was sitting in a pronounced right sideslip. The right wing was now sitting upwind, generating more lift, while the left wing sat downwind of the fuselage, reducing its lift; as a result, the sideslip tended to induce a left bank, which would cause the plane to turn left. In response, the autopilot, which had been commanded to hold their present heading, countered by using almost all of its aileron authority to bank to the right.
There was just one problem: this configuration was unsustainable. Just before embarking on the maneuver, the pilots had reduced engine power from climb to cruise, causing the speed of the airplane to decrease. As the airspeed fell, the flight controls became less effective, and the amount of right aileron needed to overpower the rudder began to increase. For 47 seconds, the autopilot was forced to slowly ramp up its right aileron input. Remarkably, no one noticed.
Then, at approximately 22:13 and 15 seconds, the autopilot reached the limit of its aileron control authority — its built-in system constraints prevented it from applying more. This caused the autopilot to disconnect automatically, illuminating a flashing red warning light. Simultaneously, the abrupt cessation of the autopilot’s right-wing-down aileron inputs caused the plane’s large right sideslip to translate rapidly into a left bank.
Feeling the plane start to roll hard to the left, Captain Adamson said, “Doesn’t like that one mate… you’d better grab it!”
First Officer Drummond reached for the controls to find that the plane was already banking steeply left, turning inward and beginning to descend. An automated voice suddenly called out, “BANK ANGLE! BANK ANGLE!”
Both pilots let out exclamations of surprise, and Drummond attempted to bank back to the right, but his inputs were ineffective. In fact, the reason they were banking left was because the left rudder input — which the rudder trim was still applying — had become too large to overcome using the ailerons.
Within seconds, the plane was completely out of control, diving downward in an extreme left bank, almost inverted. The only way to recover was to level the wings, which could only be done using the rudder, but in the chaos of the moment the pilots seemed to have forgotten that the rudder trim was still set all the way to the left. Becoming desperate, Drummond applied full right aileron and pulled the nose up, but this failed to level the plane, and in fact made the situation much worse. Pulling the nose up while sideways caused the plane to enter a terrifying spiral dive, like a piece of floating detritus being sucked down a drain. The Metroliner spun around and around, tighter and tighter, accelerating far beyond its maximum operating speed of 227 knots. The cockpit voice recorder captured a cacophony of bangs, shouts, and “BANK ANGLE” warnings. Behind the noise, Captain Adamson could be heard asking whether the autopilot was off, and Drummond replied that it was. But after that, there was a loud sound, and the recording came to an abrupt and haunting end.
At that moment, the G-forces of the spiral dive exceeded the airframe’s ultimate limit load, and the Metroliner began to break apart. Both wings snapped at the root and folded upward against the fuselage, sending the still-spinning left propeller slicing through the cabin just behind the main entry door. The tips of the wings collided with each other, then the right wing ripped off entirely, striking and severing the horizontal and vertical stabilizers as it tumbled backward. Broken electrical wires ignited fuel leaking from the shattered left wing tank, triggering a sudden explosion which lit up the surrounding clouds as the plane plunged downward, passing through 16,000 feet, at which point the flight data recorder ceased recording. At that point the left wing, now engulfed in flames, also ripped away, spiraling earthward in a halo of smoke and fire; seconds later, the fuselage, compromised by the propeller strike, ripped spectacularly in two as the cockpit broke free from the cabin. The remains of the plane, now descending in freefall, streaked across the night sky over New Zealand’s North Island, ejecting a long trail of mail and documents out into the darkness.
On the ground, local residents heard a tremendous, rising roar, prompting many of them to hurry outside to search for the source of the noise. What they saw left them speechless. A ball of fire was descending from the heavens, spewing fragments which fell to earth like flaming teardrops in its wake. The main wreckage then exploded twice more before disappearing behind a hill, at which point a loud boom was heard, followed by silence.
◊◊◊

When rescuers reached the crash site east of Mount Taranaki, they found pieces of the Metroliner strewn throughout a large sheep paddock, some of them burnt, but cold drizzle had already extinguished the flames. In one place, the fuselage lay split open, surrounded by mail; farther on, the left wing had embedded itself root-first in the ground; and beyond that were the mangled remains of the cockpit, where both pilots were found dead, having been killed instantly on impact. Although most of the large pieces were contained within a relatively small area, some lighter objects such as panels, hatches, and cargo were found up to two kilometers away, while bits of fuselage skin extended to four kilometers, and pages from the flight manual were found blowing in the wind up to 15 kilometers from the main crash site.
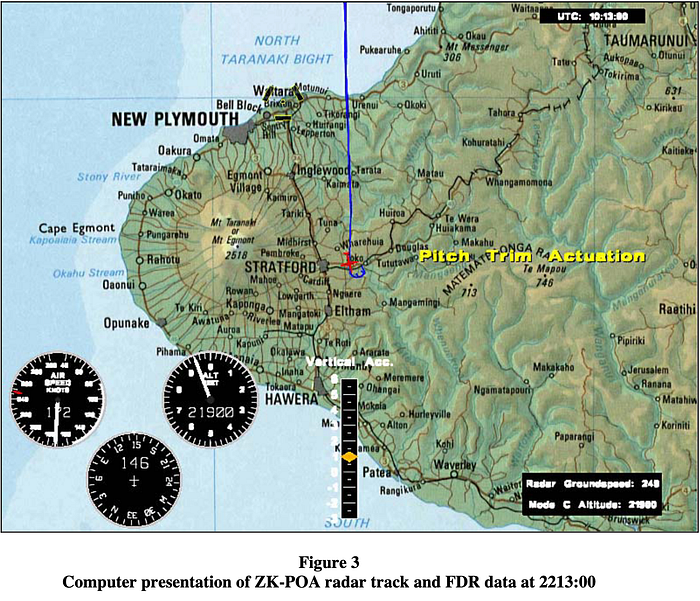
Investigators with New Zealand’s Transport Accident Investigation Commission, or TAIC, arrived on the scene the next day already knowing that Airwork flight 23 must have broken up in midair. The distribution of wreckage and the witness statements left little doubt. But what could have caused a Metroliner to disintegrate so utterly? Radar data indicated that the plane was beginning to break apart at altitudes as high as 19,900 feet, indicating that whatever brought it down unfolded rapidly. Initial media speculation focused on hazardous cargo, but an examination of the recovered mail ruled that out right away: the most dangerous thing in the cargo hold was paper.

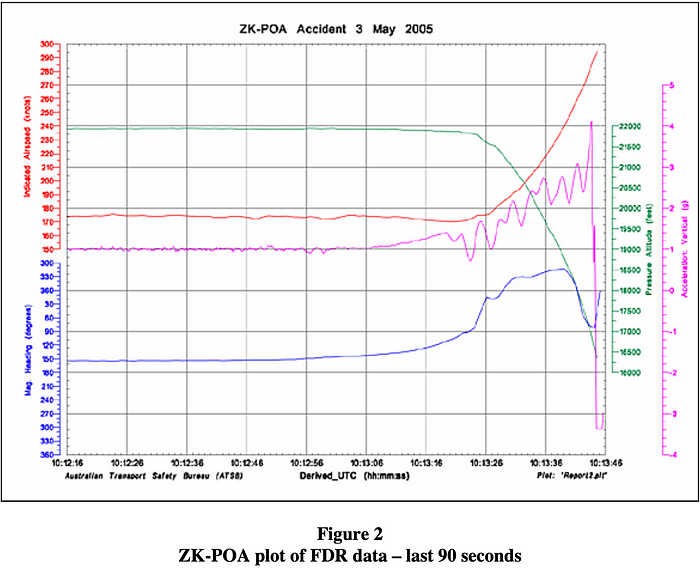
Instead, after examining the wreckage and the contents of the black boxes, the TAIC discovered that the in-flight breakup occurred because the plane exceeded its structural limitations during a tight spiral dive. By the time the flight data recording ended, the plane had achieved an airspeed of nearly 300 knots and was pulling 4.2 vertical G’s, far outside what it was built to withstand.
The TAIC also found that the sequence of events leading to this breakup began when the pilots requested that all of the fuel be placed in the left wing tank in order to save time. This was contrary to company procedures, which called for the fuel to be distributed evenly. Although the pilots did attempt to rebalance the fuel load before takeoff, this was apparently not fully successful, because Captain Adamson felt the need to rebalance it again after reaching their cruising altitude.
It bears repeating that while Airwork had been teaching its pilots how to expedite the fuel transfer process while in flight, neither the airline nor the manufacturer had an official, written procedure for this. That meant that there could be considerable variation in how individual pilots applied the technique, and indeed after interviewing other Metroliner pilots at Airwork and other companies, the TAIC found this to be the case. While most pilots said that only a small amount of rudder trim and aileron were necessary in order to “gravity assist” the fuel transfer, Captain Adamson instructed First Officer Drummond to use nearly full left rudder trim, which was unnecessary and unsafe.

Needless to say, had an official procedure been published with a suggested amount of rudder trim, the accident probably wouldn’t have happened. But there were still plenty of opportunities to prevent it. Investigators listening to the cockpit voice recording could not help but notice that First Officer Drummond seemed apprehensive about the procedure and required repeated assurances before attempting it. Despite having only 70 hours of experience on the Metroliner, he evidently understood on some level that Captain Adamson’s request was unsafe, but he never clearly articulated this, and in the end Adamson convinced him to do it.
This decision represented a failure of crew resource management, or CRM, a communication principle designed to ensure that all flight crew members take part in the decision-making process. Pilots properly trained in CRM should be able to recognize when a steep authority gradient — such as that between an experienced line check captain and a new first officer with 70 hours — might result in unequal use of human resources. In this case, First Officer Drummond either could not fully articulate his concerns or was unwilling to argue with a captain who presumably knew more than he did. As such, his opinion, despite being correct, was never shared and never considered.
It doesn’t take an aeronautical expert to understand that cruising with full left rudder trim is a bad idea, but it does take a certain sort of person to say as much when in a subordinate position. This is exactly the problem which CRM is meant to solve, but in this case it failed. In the TAIC’s opinion, the structure of Airwork’s CRM training program may have contributed to this failure, because it built up CRM skills slowly during semiannual recurrent training sessions, even though the newest and most inexperienced pilots, who have not yet been through recurrent training, are the ones who need CRM most urgently. Best practice, therefore, is to frontload CRM skills early in the training program, and had Airwork followed this format, Drummond might have had the confidence he needed to say no.

However, even after Drummond agreed to attempt the questionable maneuver, the accident still could have been avoided if the autopilot had been disengaged. In fact, the pilots should have disconnected the autopilot as soon as they climbed above 20,000 feet, per the operations manual, but they did not. The altitude limitation on the autopilot ultimately had nothing to do with the crash, but it was a missed opportunity. Alternatively, had a fuel transfer procedure existed, it would have advised the crew not to use the autopilot, for reasons which only became obvious to them in hindsight. The reason, of course, is that the autopilot does not have control over the rudder, and if the rudder trim begins to overpower the ailerons, the autopilot will simply disconnect and the plane will rapidly go out of control. On the other hand, if the autopilot is not engaged, the pilot will have to induce bank manually, and will be able to physically feel whether the amount of force required is increasing.
In the event, the pilots were likely distracted trying to determine whether the fuel transfer was working, and did not notice that the autopilot was having to apply more and more right aileron to counter the left rudder trim and keep the plane on course. The displacement of their control columns would have slowly become larger, but this would have been harder to notice in the dark. For the pilots, the first sign of trouble was the plane abruptly departing controlled flight.

Once the autopilot reached the limit of its aileron authority and disconnected, the plane began to turn left very quickly. The TAIC calculated that from the point where Captain Adamson told First Officer Drummond to “grab it,” the pilots had just 12 seconds to take decisive action before recovery became impossible. As the plane entered a spiral dive, proper upset recovery technique would have been to first reduce engine power to limit any increase in airspeed, then roll the wings level, and only then pull out of the dive. In the event, however, First Officer Drummond did not manage to reduce engine power until 18 seconds into the upset, after the plane had already exceeded its maximum operating speed, rendering recovery impossible. Furthermore, neither pilot seemed to realize that they would need to use the rudder to roll the wings level, since the rudder was what was turning them in the first place. Instead, Drummond applied full right aileron, then pulled the nose up even after this failed to level the wings. Pulling up while in a spiral dive sealed their fate, increasing the G-load on the wings until they failed.
The TAIC noted that the pilots might have been able to effect a recovery if they had received training on how to escape a spiral dive. Although Airwork did provide pilots with upset and recovery training, which in theory covers spiral dives, the capabilities of available Metroliner simulators in practice limited this training to recovery from simple nose up and nose down upsets, because the simulators couldn’t faithfully replicate aircraft behavior in extreme conditions of yaw and bank. In other cases, pilots are taught to recover from spiral dives by actually entering one in a light aircraft, but if the pilots ever did this, it was not mentioned in the TAIC’s report.

The accident highlighted an ongoing issue with the way pilots around the world on all types of aircraft were being taught to use the rudder. Most manufacturers design transport airplanes with the intention that large rudder inputs will only be necessary to counter asymmetric yaw in the event of an engine failure, or to land in a crosswind. But pilots all over the world were and always have used the rudder for other purposes, some of them safe, others less so. At Airwork, pilots should have been aware of this. In 2002, as a result of an NTSB recommendation stemming from the crash of American Airlines flight 587, the company began distributing a notice to pilots warning against the use of large rudder inputs in climb and cruise. That Captain Adamson still chose to use a large rudder input during the fuel transfer attempt despite presumably having received this notice showed that more needed to be done.
As a result of the accident, Airwork created explicit procedures for the use of the crossflow system, including that the system should not be used in the air except in the event of an engine failure. The procedure also stated the autopilot must be disconnected before initiating crossflow. Simultaneously, the New Zealand Civil Aviation Authority opened talks with the US FAA to help introduce a fuel balancing procedure into the official flight manuals for the Metroliner and other related aircraft. However, these changes did not come in time to save the sole pilot of a Metroliner which crashed in Dayton, Tennessee in 2006, apparently due to a loss of control while attempting to rectify a fuel imbalance.

As far as direct implications go, the crash had relatively few: it was little more than a footnote alongside deadlier disasters involving larger airplanes, and most pilots probably haven’t heard of it. Nevertheless, Airwork flight 23 is worth highlighting because it underscores many of the most important aspects of safe flying which pilots should know. On the most fundamental level, the accident was caused by the pilots’ attempt to solve a problem which was not really that serious. In fact, the technique used to solve it was much more dangerous than the problem itself, and that, if anything, is where they went wrong. Every pilot needs to be able to take a step back, think about the situation, and assess relative levels of risk independently of the weight they may attach to a particular goal. Even though the procedure may or may not have been normalized at the company, common sense should have revealed it to be dangerous. This type of thinking could have prevented the crash of Airwork flight 23, and has prevented countless other accidents which we will never hear about.
There were, of course, plenty of other factors, including the lack of a written fuel transfer procedure, the informal and mission-oriented company culture, and the unusual design of the Metroliner’s fuel system. But this accident is best framed as a lesson on decision-making. A routine mail flight fell to pieces over New Zealand because of a series of decisions, each building on the last, which could have been reversed at any time, but was not. Sometimes, the difference between a normal flight and a fiery death could be as simple as asking, “Why are we doing this?” If only this question were asked more often, a lot more pilots would still be alive.
_____________________________________________________________
Join the discussion of this article on Reddit!
Visit r/admiralcloudberg to read and discuss over 200 similar articles.
You can also support me on Patreon.
