Lessons of Another Age: The crashes of United Airlines flights 608 and 624
On the 24th of October 1947, a United Airlines Douglas DC-6 caught fire over Utah, forcing the pilots into a desperate battle to get their burning plane on the ground. But just moments before landing at a remote airfield, the flight controls failed and the plane smashed into the edge of a plateau in Bryce Canyon National Park, killing all 52 passengers and crew on board.
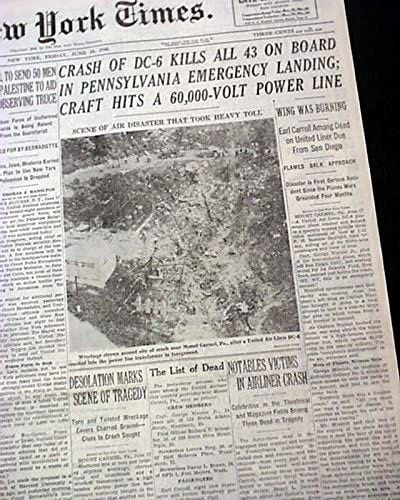
Eight months later, on the 17th of June 1948, another United Airlines DC-6 crashed near Mount Carmel, Pennsylvania after the pilots reported a fire in the cargo hold. All 43 people aboard perished when the pilots were overcome by CO2 from the fire extinguishing system, causing them to lose control of the plane.
As it turned out, these two crashes were intimately connected — one had in fact led directly to the other, as an attempt to correct a deadly design flaw introduced another in its place. Both problems were emblematic of a time when aviation safety was still in its infancy, when the dawn of powered flight had not yet faded from memory. But both crashes were also eminently preventable. In the lead-up to the two accidents, warnings were ignored, dangerous shortcuts were taken, and pilots were left in the dark — all because of a deliberate effort to create an impression of safety where none in fact existed. And yet the twin tragedies of United Airlines flights 608 and 624, as senseless as they were, would also lead to the implementation of basic safety measures that are taken for granted today. For that reason alone, it is worth diving 74 years into the past to take a look back at how it all began.
◊◊◊
In 1947, the jet era was but a glimmer in the eyes of futurists, and the greatest of the propliners had only just begun their long and glorious terms of service. The first widely used pressurized airliners had only entered service four years before, and the wide open skies above 10,000 feet were the domain of a handful of prestigious four-engine giants and the heroic pilots who flew them. One of these planes was the Douglas DC-6, a brand new passenger plane powered by four huge radial piston engines, which first entered service in early 1947 with American and United. The DC-6 would seem tiny in today’s world of wide-body jets, but in 1947 it was considered a beast at over 33 meters in length and with room for up to 68 passengers. It could fly from Los Angeles to New York or from New York to London without stopping, a feat which few other planes could match at the time.

On the 24th of October 1947, a few months after the introduction of the DC-6, 47 passengers and five crew boarded United Airlines flight 608, a scheduled non-stop service from Los Angeles to Chicago. Nearly everything about their experience would be unrecognizable today. Aboard the DC-6 “Mainliner,” they could expect to enjoy large, plush seats with plenty of legroom (for overnight flights, they could even convert into bunks); unlimited smoking; and comprehensive in-flight meal service; but on the other hand, they could also expect only very limited safety equipment, most of which was explained on a pure text safety card without any pictures. The pilots too were built different: Captain Everett McMillan and First Officer G. G. Griesbach could barely scrape together a combined 200 hours on the DC-6, in part because the plane had only been in service for a few months, but also because training requirements in 1947 were much less stringent. Captain McMillan’s 15,000 total hours on other aircraft types were judged sufficient for him to transition directly to the position of commander on the DC-6 after completing a brief introductory course.
At 9:23 a.m. local time, flight 608 departed Los Angeles and proceeded to its cruising altitude of 19,000 feet, headed northeast over the vast Mojave Desert. In those days there was no national air traffic control network; instead, while en route the pilots communicated with company dispatchers only, to whom they reported passing certain waypoints marked on their charts. Over the next two hours the pilots reported crossing Fontana, Daggett, Silver Lake, Las Vegas, and Saint George, placing them somewhere over southwestern Utah, although nobody knew precisely where because there was no radar. The crew did however report that they expected to cross the Bryce Canyon waypoint at 12:22. That put them over a remote area of the Colorado Plateau dominated by ruddy wastelands, forested buttes, and otherworldly rock formations largely devoid of human habitation.
It was here, at 12:21, that Captain McMillan suddenly reported a fire in the baggage compartment. He had activated the fire extinguishers, he said, but the fire kept growing; smoke was filling the cabin, and he was going to make an emergency landing. The only possible landing site was Bryce Canyon Airport, an airfield constructed in the 1930s to serve the nearby National Park of the same name. The airport was rarely used by commercial airliners, but it would have to do.

As the DC-6 made an emergency descent over the desert, witnesses caught sight of the airliner overhead with flames and white smoke pouring from its right wing root. Captain McMillan radioed dispatch again and said, “tail is going out — we may get down and we may not,” an ominous transmission which suggested that the fire was eating through the cables that allowed him to move the control surfaces on the tail, including the elevators.
48 kilometers out from Bryce Canyon, the smoke turned black and objects began to fall from the plane, including pieces of fuselage skin, baggage, the main cabin entry door, an alcohol tank, and the trailing edge of the right wing flap. Still the plane hurtled onward, her cabin filled with smoke and flames, her pilots struggling with their dying controls. Bryce Canyon Airport hove into view in the distance, their last, best hope of salvation. United dispatchers heard Captain McMillan say, “We may make it — approaching a strip!” But after that, no more was heard.
Less than a kilometer southeast of the airport, the controls at last failed, and flight 608 entered an uncontrolled, spiraling turn. The plane just cleared the rim of Bryce Canyon before slamming into the top of the plateau at great speed, carving out a crater and sending burning debris cartwheeling through the sage brush desert for several hundred meters. By the time emergency crews arrived at the scene, the only recognizable piece of the DC-6 was its battered tail, and it was clear that none of the 52 people on board could have survived. At the time it was the second deadliest plane crash in US history.

United Airlines flight 608 had come down just inside Bryce Canyon National Park, a few meters south of the main road which ran up from the town of Tropic to the park headquarters and visitor center. There were, however, no witnesses to the crash itself. That left the Civil Aeronautics Board, the agency then responsible for investigating air crashes, without much to go on. Black boxes hadn’t been invented yet and there was no radar which could have tracked the path of the airplane, leaving them with only the wreckage itself and the communications between the pilots and United dispatchers. Furthermore, air crash investigation as a discipline had only existed for ten or fifteen years and the extant body of knowledge was rudimentary at best. In newspaper articles from the days after the crash, it was thus widely assumed that the cause of the fire which brought down United 608 probably would not be found.
Over the two weeks following the crash, CAB investigators collected wreckage from the crash site and sent search parties out into the desert to scour the flight path, turning up numerous pieces of debris as far as 48 kilometers from the site of the accident. The debris was then transported to a hangar in Santa Monica, California, where the CAB began to reassemble the plane to try to determine how the fire spread. One thing soon became apparent: although the pilots had reported a fire in the baggage compartment, the fire clearly began elsewhere and spread into the hold once it was already well advanced. The crew simply reported a fire in the hold because this was the first affected area equipped with a fire alarm, which also explained why the fire did not go out when they activated the fire extinguishers in the baggage compartment.
CAB investigators had only just begun to piece together the actual origin of the fire when another DC-6 ran into trouble. On the 11th of November 1947, a DC-6 operating an American Airlines flight from San Francisco to Chicago caught fire over Arizona and made an emergency landing in Gallup, New Mexico. Fortunately, the pilots were able to get the plane on the ground, and all 25 passengers and crew evacuated safely before the fire consumed the cabin. With two cases of brand new DC-6 airplanes having been destroyed by fire in a period of less than three weeks, Douglas Aircraft took the difficult decision to ground every DC-6 in America later that same day. Airlines scrambled to find new planes to cover core routes, as did President Harry Truman, who used a DC-6 as the presidential aircraft.
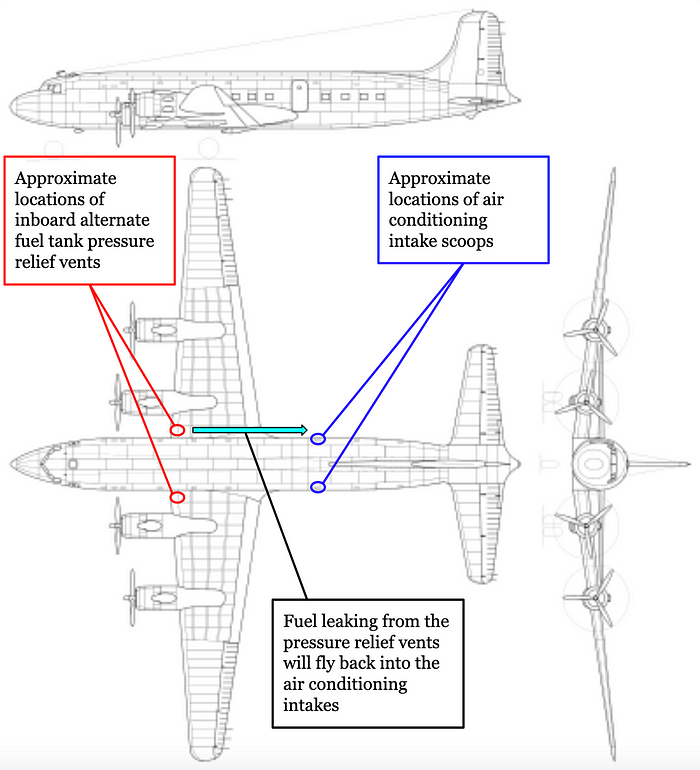
The relatively intact state of the airplane which landed at Gallup provided CAB investigators with a lucky break. The distribution of scorch marks and soot deposits showed that the fire on this aircraft developed in a similar manner to the fire which brought down United 608 at Bryce Canyon. By tracing back the series of stains and burn marks, CAB investigators were able to show that in both cases fuel leaked out of a vent underneath the leading edge of the right wing near where the wing attached to the fuselage; flowed backwards in the slipstream; and was sucked into a scoop on the lower fuselage that served as the air intake for the cabin air conditioning system. Fuel vapors flowed into the system until they reached the cabin heater, causing it to backfire; the fuel then ignited and set fire to the ducting inside the air conditioning chamber. From there the fire spread both along the outside of the fuselage and through the cabin interior.

On United Airlines flight 608, the fire next proceeded into the baggage compartment, triggering the first fire alarms; around the same time, smoke must have poured into the cabin through the air conditioning vents, and later in the flight open fires were likely burning in the passenger area. Although autopsies could not be conducted due to the fragmentation of the bodies, it was thought that most of the passengers probably perished while the plane was still in the air. The key difference between the Bryce Canyon crash and the near miss at Gallup appeared to have been the fact that United 608 was carrying several barium nitrate emergency landing flares in a compartment inside the cabin. (In the days before electronic locator beacons and continuous radar coverage, flares were the primary method by which survivors of a crash could alert rescuers to their location.) When the fire reached this compartment, the flares ignited and greatly increased the intensity of the fire, ultimately leading to the destruction of the cables which allowed the pilots to move the pitch control surfaces. The American Airlines flight, by contrast, did not carry any emergency landing flares, and the pilots consequently had enough time to get their plane on the ground with all its occupants still in one piece. But one critical question remained: how did fuel leak from the tank in the first place?
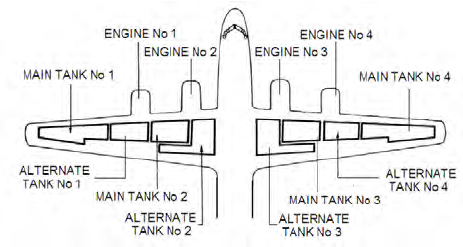
Understanding how this might have happened requires a brief explanation of the DC-6’s fuel system. The Douglas DC-6 has eight fuel tanks in the wings, consisting of one main tank and one alternate tank for each of its four engines. Two auxiliary tanks can be used to further increase fuel capacity, but they were not used on flight 608.
While in flight, it was common practice to run the engines off the main tanks during climb, switch all the engines over to the alternate tanks during cruise, then change back to the main tanks once the alternate tanks ran low.
To control which tank provided fuel to the engines, the cockpit featured four fuel source selectors, one for each engine. There were also two cross-feed selectors which allowed engines to draw fuel from a tank belonging to a different engine. For example, to run both engines on the right wing off the #3 alternate tank, the pilots could set the #3 engine fuel source selector to “alternate,” the #4 engine fuel source selector to “off,” and the right cross-feed lever to “on engines three and four,” opening up a fuel line from the #3 alternate tank to the #4 engine. Using various combinations of lever positions, it was therefore possible to run any two engines off of any of their four associated fuel tanks.
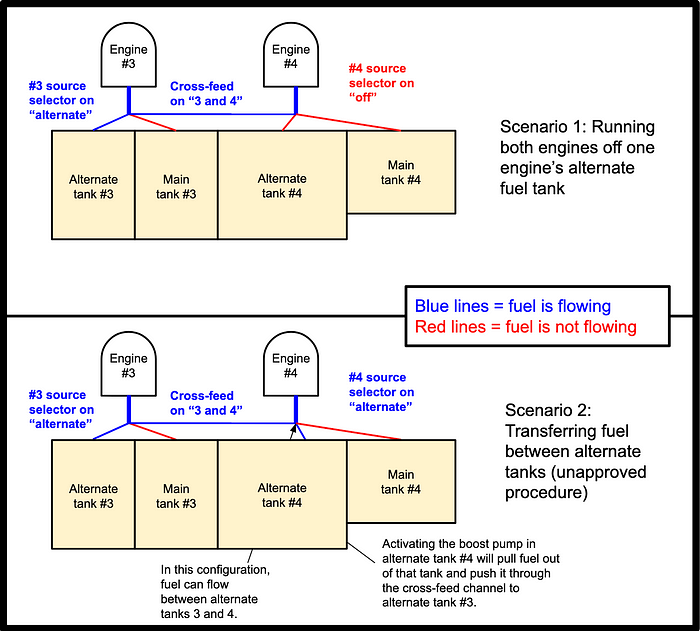
However, pilots who flew the similar Douglas DC-4 had learned that it was possible to use this system to transfer fuel between the tanks themselves, a practice which still worked on the larger DC-6. Although the plane was not designed with the intent to allow fuel transfer, it was relatively easy to do so. For example, in order to transfer fuel from the #4 alternate tank to the #3 alternate tank, pilots could leave both the #3 and #4 fuel selectors on “alternate,” set the right cross-feed to “on engines 3 and 4,” and turn on the boost pump for the #4 alternate tank. The key difference between this and the procedure described in the previous paragraph was that with the #4 fuel source selector set to “alternate” instead of “off,” the #4 alternate tank was still hooked into the fuel system. Therefore when the cross-feeds were opened, fuel had a channel through which it could move between the #3 and #4 alternate tanks, while the boost pump served to force fuel through that channel. The exact same thing could also be done with the #1 and #2 tanks in the left wing.
But because the fuel system was not designed to allow for fuel transfer between tanks, there was nothing stopping a pilot from pumping fuel into an already full tank until it overflowed. If this were to occur, the excessive fuel pressure inside the tank would cause fuel to force its way out through that tank’s pressure relief vent. All fuel tanks had pressure relief vents to ensure that the air inside the tanks could escape as the airplane climbed, maintaining equal pressure inside and outside the tank. But if the tank reached its capacity and the boost pump kept injecting more fuel into it, the fuel would begin to escape through this pressure relief vent at a rate of 47.3 liters per minute. If fuel leaked out of the relief vents for the four main tanks or the #1 and #4 alternate tanks, there would be no particular danger, but the vent outlets for the #2 and #3 alternate tanks were positioned such that escaping fuel would be carried by the slipstream directly into the air conditioning intakes, where it would contact the cabin heating system, virtually guaranteeing a fire.
As it turned out, pilots regularly transferred fuel in this manner, even though there was no procedure for it in the operations manual. They had in fact learned the technique by word of mouth from Douglas’s own training pilots while the DC-6 was being introduced to the fleet, despite the fact that Douglas’s official policy was that fuel transfer was not allowed. But while the manual did not provide a fuel transfer procedure, it didn’t explicitly prohibit it either.
The CAB was quick to note that because of this vulnerability, the Douglas DC-6 clearly did not meet CAA certification requirements, which stated: “In the case of systems with tanks whose outlets are interconnected, it shall not be possible for fuel to flow between the tanks in quantities sufficient to cause an overflow of fuel from the tank vent when the airplane is operated as specified in 04b.4221 (a) and the tanks are full.” During certification, one of the questions on the CAA inspector’s checklist also read, “Do vents appear to terminate where the discharge of fuel vent outlet will not constitute a fire hazard? Yes/No,” on which the inspector had circled “yes,” although this was in fact false, as the two in-flight fires attested. Douglas and the CAA explained that they had not envisioned that fuel would ever escape through the relief vents, thus there was nothing to constitute a fire hazard; although it turned out that it was possible to cause this to occur simply by manipulating the fuel system controls. Douglas had not detected this vulnerability because it didn’t actually conduct any tests to determine whether fuel transfer was possible or whether the fuel tanks could be over-pressurized.
The final piece of the puzzle was why fuel was transferred into the #3 alternate tank in sufficient quantity to cause it to overflow. According to a CAB summary of testimony from a copilot who usually flew with the captain, McMillan frequently transferred fuel in order to equalize the fuel levels across all four alternate tanks. After reaching cruise altitude, he would run all the engines off their alternate fuel tanks, until one of the tanks reached a minimum of 500 pounds (227kg). He would then set all the fuel selector switches to alternate, place the left and right cross-feeds in the “on engines 1 and 2” and “on engines 3 and 4” positions respectively, and set the boost pumps in alternate tanks 1 and 4 to “high.” The CAB noted that if the captain forgot to switch off the #4 boost pump once the amount of fuel in the #3 and #4 alternate tanks was equalized, it would just keep pumping fuel into the #3 tank until it overflowed.
When I originally wrote this article, I thought that this didn’t make any sense, because in most versions of the DC-6, the #2 and #3 alternate tanks were bigger than the #1 and #4 alternate tanks, which were closer to the tips of the tapered wings. As a result, I struggled to understand why a pilot would transfer fuel from outboard to inboard while equalizing the fuel levels, given that the outboard tanks should run low first.
However, in 2025 I discovered that there was one version of the DC-6 where the outboard alternate tanks were larger than the inboard alternate tanks, and circumstantial evidence led me to believe that this was almost certainly the fuel tank format on the accident airplane.
Given that the #4 alternate tank was in fact bigger than #3, it would have been possible to inadvertently overfill the #3 alternate tank while transferring fuel if the fuel transfer was started when the #4 tank was still more than half full. (That’s because the volume of fuel remaining in the #4 tank needs to be greater than the volume that has been consumed, or else the #3 tank won’t overflow.) Overflow could then occur if someone inadvertently left the boost pump in the #4 alternate tank running for too long.
Most likely, the technique of equalizing fuel levels was a workload saving shortcut. Because the alternate tanks weren’t all the same size, normal procedures required the pilots to monitor the fuel levels in the alternate tanks very closely in order to switch all engines to run off the larger outboard alternate tanks once the smaller inboard tanks ran low, while making sure not to leave too much fuel behind in those tanks either. This monitoring and configuration change would then have to be repeated when the outboard alternate tanks ran low as well. On the other hand, equalizing the fuel levels could be undertaken at any time, without waiting for any particular fuel level to be achieved, which was more convenient. Furthermore, it would cause all the alternate tanks to run empty at the same time, eliminating the need to set up a crossfeed.
◊◊◊
Following the crash and the near miss, the DC-6 remained grounded for four months while Douglas implemented a wide range of design changes, including improved fire extinguishers, a redesigned cabin ventilation system, better fire protection around the emergency flares, check valves to prevent the pilots from transferring fuel, smoke detectors in the air conditioning chamber, and a new location for the alternate fuel tank relief vents. The operations manual was also updated to explicitly prohibit the transfer of fuel between different tanks. Following the changes and their approval by the CAA, the CAB wrote, “The investigation has disclosed the cause of these accidents so precisely and the required modifications have been so extensively accomplished that there is no reason to doubt that the causes of these accidents have been effectively eliminated through such modifications.” In March 1948, the DC-6 was cleared to fly again, and by June it had re-entered service with major US airlines.
And the story should have ended there, with the DC-6 fleet flying off into the sunset for a long and safe flying career. But tragically, it did not.
In early 1948, Douglas engineers were testing the interaction of the new ventilation system with the DC-6’s improved banks of CO2 fire extinguishers when a disturbing incident occurred. After activating the extinguishers to put out a simulated fire, high concentrations of carbon dioxide flowed back into the cockpit from the baggage compartment, causing the partial incapacitation of the flight crew, who nearly lost control of the airplane before regaining consciousness. A CAA inspector and a representative of the pilots’ union were also on the plane at the time and witnessed the near-catastrophe. The incident prompted Douglas to install a relief valve in the ventilation system which could be activated before releasing the fire extinguishers in order to reduce the amount of CO2 that entered the cockpit. The company also hired Dr. Clayton White, a medical specialist, to review the tests and compile known research into the effects of CO2 on the human body.
CO2 displaces oxygen in the air, causing suffocation, and is also toxic in large concentrations. However, in 1948 it was not known with any certainty how much CO2 had to be present in the air before conditions became unsafe. Dr. White concluded that the most reliable data seemed to indicate that CO2 concentrations above 5% would be hazardous. He also concluded that Douglas’s tests following the installation of the new relief valve were woefully inadequate to determine whether CO2 concentrations would stay below this threshold, because Douglas didn’t monitor the concentrations carefully enough, didn’t set off all the extinguishers simultaneously, and didn’t conduct tests in all of the approved emergency descent configurations. White wrote that Douglas should rerun the tests more carefully in order to “avoid some embarrassment at a future date,” and recommended that Douglas share the report with the CAA, the Airline Medical Doctors’ Association, and the Air Transport Association.
But instead of following Dr. White’s advice, Douglas’s chief test pilot wrote “do not discuss with CAA” on the cover of the report and filed it away from prying eyes. Subsequently, the CAA approved the changes to the design of the DC-6, certifying that they met federal requirements, without realizing that a consultant hired by Douglas had deemed their tests insufficient to demonstrate compliance. The only safeguards were the relief valves and a line in the fire response checklist reminding pilots to open the valves before releasing the extinguishing agent in order to prevent “excessive” CO2 buildup inside the plane. (The CAA originally wanted them to use the word “lethal,” but Douglas convinced the agency to let them use “excessive” instead, apparently in order to avoid the impression that the fire extinguishing system was dangerous.)
Then, on May 13th 1948, a TWA Lockheed Constellation experienced a spurious fire warning which prompted the crew to activate the CO2 extinguishers in the forward baggage compartment. As they entered an emergency descent, CO2 leaked from the hold and pooled in the cockpit, causing the pilots to become partially incapacitated. Fortunately, they were able to recover and make a safe landing in Chillicothe, Missouri. After a month-long investigation, the Air Transport Association, an airline interest group, sent a telegram to all operators of the Douglas DC-6, informing them of the circumstances of the incident, discussing what could be done to recover from such a situation, and warning that they had reason to believe a similar event could occur on the DC-6. The telegram concluded by recommending that operators conduct tests to find out whether this was in fact the case.
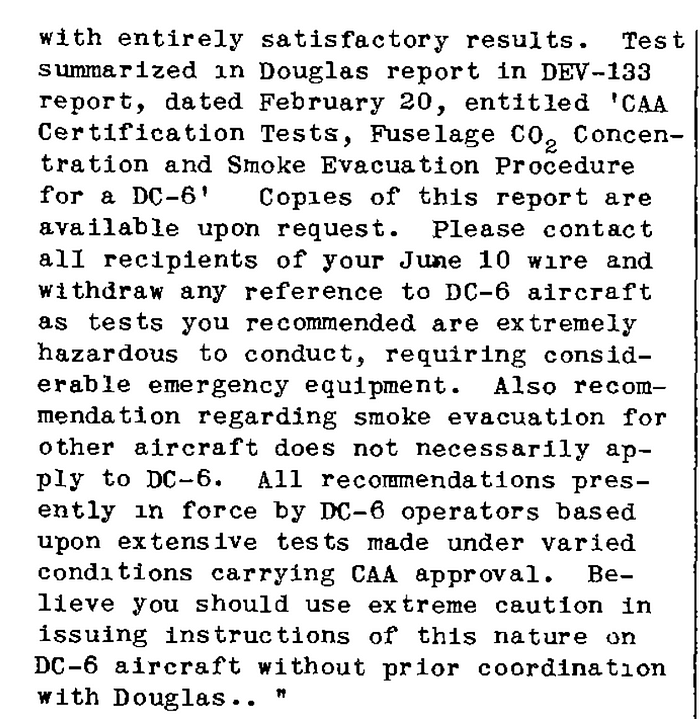
On June 15th, the Douglas Aircraft Company replied with a terse telegram of its own. Douglas demanded that the ATA contact all recipients of the original telegram in order to withdraw any reference to the DC-6, since Douglas had already carried out such tests with “entirely satisfactory results;” besides, it argued, the tests were quite hazardous and it was unwise to recommend that airlines perform them. The company concluded by writing that its own recommendations for dealing with CO2 in the cockpit were “based upon extensive tests made under varying conditions carrying CAA approval,” and that the ATA should not be recommending solutions which may not be equally applicable to different aircraft. Later that day, the ATA caved to Douglas’s demands and sent out a new telegram informing all DC-6 operators that the plane had been adequately tested to ensure that dangerous concentrations of CO2 could not occur.

Two days later, on the 17th of June 1948, United Airlines flight 624, another Douglas DC-6, departed Chicago, bound for New York. In command were Captain George Warner, who only had about 30 hours on the DC-6, and First Officer Richard Schember, who had 129. Two flight attendants and 39 passengers also boarded the midday flight. Due to Douglas’s obfuscation, none of them had the faintest knowledge of the deadly flaw which lurked within the modified DC-6.
The first couple hours of the flight proceeded without incident, until the plane arrived over eastern Pennsylvania. As they cruised at 17,000 feet, the pilots suddenly received a warning of fire in the forward baggage compartment. There was in fact no fire, but they could not have known this.
One of the pilots managed to send off a garbled, panicked message to LaGuardia: “624… 624… Fire. Discharging [unintelligible] forward baggage pit…”
“Can’t hear, try again, please,” the controller said.
“624, emergency!”
Another pilot heard what sounded like screaming, following by someone yelling, “This is an emergency descent!”
“Can’t hear, try VHF!” the controller said again.
“624,” said the pilot, “coming down, I… ah… ah…” And then there was silence.
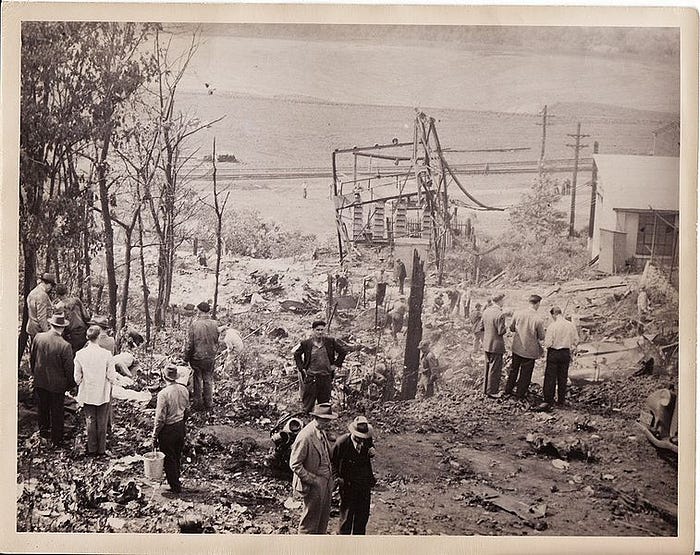
No further transmissions were heard from United Airlines flight 624, but the plane kept flying for another ten minutes. The DC-6 passed over Sunbury Airport at 4,000 feet but made no attempt to land, then entered a left turn near the town of Shamokin while descending between 500 and 1,000 feet above the ground, heading into a mountainous area. The plane was seen again several minutes later near Mount Carmel, where it flew within 200 feet of the ground, then entered a climbing right turn towards high terrain. Moments later the plane slammed into a transmission line clearing on the side of a wooded mountain, destroying a 66,000-volt transformer and severing power lines before it struck the ground and disintegrated, spewing debris several hundred meters up the mountainside. Witnesses rushed to the scene to help, but it was obvious that no one could have survived; all 43 passengers and crew had perished in the fiery impact.
At LaGuardia, the controller asked a nearby United flight if they could see flight 624, as the plane was not responding to transmissions. Chillingly, the pilot replied, “Flight 624 stands in no further need of assistance — wrecked at Mount Carmel.”
Based on the transmissions picked up by LaGuardia, it was clear that the pilots thought they had a baggage fire and had discharged the fire extinguishers. However, examination of the wreckage showed that no fire had occurred prior to impact; the warning was in fact false. This was not unusual; already in 1948 there had been 22 false fire warnings on US airliners and over 280 false smoke warnings, far more than the number of real fire and smoke events. It was actually the attempt to extinguish this imaginary fire that led to the accident. Witness marks left on the relief valves at the moment of impact showed that they were closed — in their panic to extinguish the fire, the crew had forgotten to open them. Tragically, United Airlines’ version of the fire checklist omitted the warning about the consequences of not opening the valves, making this step much easier to gloss over. There was no way to know exactly what happened aboard the plane following this error, but the absence of further transmissions, the erratic flight path, and the fact that the crew apparently overflew several suitable landing sites suggested that the crew were partly or totally incapacitated by CO2 during those harrowing final minutes.
Subsequent investigation by the CAB showed that even with the relief valves open, in certain descent configurations CO2 concentrations in the cockpit could still reach dangerous levels. In the case of flight 624 the valves were probably closed and evidence suggested that the plane was probably not in the aforementioned configuration, but the findings only reinforced Dr. Clayton White’s admonition that Douglas’s tests were inadequate to ensure that the airplane was safe. Only much later, during a lawsuit filed against Douglas and United by the family of one of the victims, was White’s report revealed. Its submission as evidence led to a scandal of its own, when the judge penalized Douglas’s defense lawyer for attempting to erase the words “do not discuss with CAA” from the front cover.

The investigation also found that in March 1948, the Air Line Pilots’ Association had lobbied the CAA to require full face, pure oxygen masks for airline pilots, citing the fact the existing rebreather-type masks, which mix oxygen into the surrounding air, could not protect against smoke or toxic gases such as CO2. However, the CAA rejected the proposal, arguing that existing procedures for clearing smoke and gases from the cockpit were already sufficient and that pure oxygen masks were not needed. Following the tragedy at Mount Carmel, the CAA quickly reversed course, mandating that all airliners be equipped with pure oxygen masks and requiring that pilots put them on before activating fire suppression systems. Such masks are still standard on every aircraft today, but they came too late to prevent the crash of flight 624.

In the wake of the accident, Douglas Aircraft changed the design of the DC-6 so that pulling the fire extinguisher handles would automatically open the relief valves to keep CO2 out of the cockpit. In its final report, the CAB made the astute observation that humans cannot be relied upon to perfectly follow a multi-step procedure in an intense emergency situation, and that a single button which activates multiple emergency systems, such as that installed by Douglas after the accident, is a much more effective way to prevent human error. For this reason, all aircraft systems today are designed from the start with this principle in mind.

In a different era, this sequence of preventable accidents might have irreversibly harmed the reputation of the airplane. But within a few short years, Douglas’s role in the crashes had been forgotten, and the DC-6 went on to become one of the most successful airplanes of its era, with over 700 built before production ended in 1958. Some of them are still flying today with Everts Air Cargo in the Alaskan far north, apparently quite safely. But the fact remains that Douglas Aircraft chose to get there the hard way, fighting at all costs to maintain an impression of safety without ensuring that their flagship airplane was actually safe. Better testing of the fuel system could have prevented the crash of flight 608, and the crash of flight 624 could also have been prevented if Douglas had listened to the experts it hired. Douglas apparently learned very little from these lessons, as its planes continued to suffer from catastrophic and preventable design flaws well into the jet era. On the other hand, the aviation industry as a whole learned quite a lot, leading to changes in the way every airliner is equipped and designed. Back then, aviation safety was a vast unexplored frontier full of both deadly dangers and innovative solutions. And when we look back at that era of aviation, an era that in a few short years even the oldest among us will cease to remember, it is worth appreciating how far we have come.
_________________________________________________________________
Join the discussion of this article on Reddit!
Visit r/admiralcloudberg to read and discuss over 200 similar articles.
You can also support me on Patreon.
