Man vs. Runway: The crash of American Airlines flight 625
On the 27th of April 1976, the town of Charlotte Amalie in the US Virgin Islands witnessed one of the territory’s worst ever disasters when an American Airlines jet overran the runway and slammed into a gas station, killing 37 people and wounding dozens more. The crash occurred during an ongoing controversy about the island’s airport, which was known for its short runway, gusty winds, and steep surrounding terrain. Was the crash, as some publications later contended, “bound to happen?” That question would form the unspoken center of the subsequent investigation, which revealed a normal landing that suddenly went wrong, forcing an experienced captain to make a split second decision: try to stop, or go around? The investigation, as was typical for inquiries in that era, did a relatively thorough job of explaining what happened, but not necessarily why, touching only briefly on the deeper reasons behind the captain’s incorrect decision and the systemic factors which caused him to make it. Examining those factors from a modern perspective allows us to confront the most important question of all: are pilot errors inevitable, and if so, whose job is it to mitigate them?

◊◊◊
Far to the southeast of Florida, off the east coast of Puerto Rico, lie the US Virgin Islands, an unincorporated US territory home to some 87,000 people scattered across several rocky islands in the Caribbean. Ever since WWII, when the first airport was carved into the precipitous coast of the island St. Thomas, the Virgin Islands have been a popular tourist destination, drawing hundreds of thousands of visitors from the US and around the world with their beaches, resorts, and excellent climate.
The local inhabitants have long had a love-hate relationship with the vast numbers of tourists on which their economy relies, and the airport has become the focus of this energy at several points during the last 60 years. The field, once known as Harry S. Truman Airport and now named for former Virgin Islands governor Cyril E. King, lies just outside the territory’s capital of Charlotte Amalie, tucked in between the waters of Brewers Bay and the steep, forested hills of St. Thomas Island. In 1976, its single runway was only 1,420 meters (4,658 feet) long, unusually short for such a busy airport, and controversy had been ongoing for many years concerning its length. Was it too short? Should it be extended? Locals and pilots alike feared disaster if passenger jets continued to land there, but expansion plans got tied up in local politics. Although Charlotte Amalie on St. Thomas Island was the capital and prime tourist destination, the majority of the population of the Virgin Islands lived (and still lives) on the larger and flatter island of St. Croix, some 65 kilometers to the south, which was also equipped with a bigger airport and a longer runway. The inhabitants of St. Croix claimed they had a better solution than leveling a hill or filling in a bay to extend the runway on St. Thomas: the jets, and the tourists on them, should simply fly to their island instead.
The dispute had not been resolved when, on the 27th of April 1976, American Airlines flight 625 departed Providence, Rhode Island, bound for Charlotte Amalie with a stopover in New York City. In command of the Boeing 727–100 operating the flight were three pilots highly experienced in Caribbean operations. In the left seat was 54-year-old Captain Arthur “Art” Bujnowski, a former US Navy pilot with 22,000 flight hours and 154 previous landings on St. Thomas. He was joined by 36-year-old First Officer Edward Offchiss, who had 8,000 hours and 38 trips to St. Thomas, and 45-year-old Flight Engineer Donald Mestler, who had flown to St. Thomas 125 times during his 9,500 flying hours.
Given their experience, the pilots would have been quite familiar with the numerous exigencies of landing on St Thomas. In 1971, shortly after its acquisition of Trans Caribbean Airways and the accompanying 727 service to Charlotte Amalie, American Airlines had issued a bulletin to flight crews listing all of the hazards and special procedures associated with landing there. The bulletin noted that high terrain near the airport interacted with the trade winds out of the east to create a standing “mountain wave” directly over the airport whenever the wind speed exceeded 15 knots, and other forms of turbulence were common. The airline required that approaches be flown by the Captain, and only onto runway 9, noting that approaches to runway 27 — the same runway in the opposite direction — were prohibited due to high hills just east of the airport. The bulletin also stated that 727 pilots must extend the flaps to 40 degrees, allowing for lower approach speeds, unless there were “strong, gusty winds,” in which case the captain could choose to use 30 degrees of flap instead.

With 81 passengers and seven crew aboard, flight 625 departed New York’s John F. Kennedy International Airport at noon on the dot, expecting to arrive in Charlotte Amalie in a little over three hours. The weather that day was benign, with few clouds and only a moderate 10- to 12-knot wind out of the southeast, providing relatively good conditions for the approach.
Shortly before 15:00, already more than half way through its descent, flight 625 encountered the first minor hiccup on what should have been a normal approach. As the plane passed through 10,000 feet, an anomaly occurred in the cabin pressurization system, causing an uncomfortable pressure spike. Passengers and crewmembers allegedly experienced ear pain and temporary deafness, as did the crew, who tried their best to mitigate the issue using the manual pressurization controls. As Flight Engineer Mestler worked on the problem, Captain Bujnowski commented, “Boy I’m deaf — I can’t hear a goddamn thing.”
“Yeah,” said First Officer Offchiss. “The bloody thing hurts, my ears hurt.”
“I hope nobody…” Bujnowski started to say.
“No, they won’t,” said Mestler.
At question, presumably, was whether the passengers would complain. In an effort to avoid such an eventuality, Captain Bujnowski asked air traffic control to cancel their IFR (instrument flight rules) clearance, allowing them to proceed visually toward the airport at whatever rate of descent they liked. The request was granted, and Bujnowski pulled back to slow their descent rate, and with it, the rate of increase of the cabin pressure.

Meanwhile, the pilots began to configure the plane for landing. Bujnowski elected to use 30 degrees of flap, because in his experience any wind out of the southeast was likely to create gusty conditions, and he found the plane to be more controllable in turbulence with the flaps at 30 degrees instead of 40. He also picked an approach speed 10 knots above the reference speed, probably to assist in penetrating turbulence.
At 15:10, with airport in sight and all checklists complete, they were on course and seemingly headed for a successful landing. Passing through 120 feet above the ground, Bujnowski commented, “Right about here’s where we hit that stuff,” presumably referring to turbulence. The plane’s airspeed rose and then fell as a gust of wind washed over it, but Bujnowski held steady on the approach course.
“A hundred,” First Officer Offchiss called out. Moments later, the plane crossed the runway threshold at a height of 80 feet, slightly high but still on track to land within the designated touchdown zone. Nearby pilots and air traffic controllers, watching flight 625 from a variety of vantage points, saw nothing out of the ordinary.
“Fifty,” Offchiss said. Bujnowski began to pull the nose up, initiating the landing flare. “Forty. Thirty. Twenty. Ten…”
Just as the plane was about to touch down, a gust of wind struck it from the front left quadrant, sending the 727 rolling sharply to the right. Captain Bujnowski let out an exclamation of surprise and turned his yoke hard to the left to prevent the right wing from striking the ground. But when the plane leveled out, it was still at 10 feet, floating along just above the runway surface without quite touching down.
Five seconds after the gust of wind, First Officer Offchiss said, “Still high, Art.”
Realizing that they had not yet touched down, Bujnowski immediately pushed the plane onto the ground, only to second guess himself just as the wheels made contact. They had touched down more than half way down the runway, and the remainder was disappearing fast. Suddenly realizing that he wouldn’t be able to stop, he reversed course and announced, “Let’s go around!”

Abandoning the landing, Bujnowski immediately pushed the thrust levers up to the half way point, per the American Airlines go-around procedure, and waited to see if thrust would increase. After a couple seconds, he still hadn’t heard a change in the sound of the engines or felt any acceleration, so he increased thrust even more, all the way to the stop.
“Flaps 25?” Offchiss asked.
“Flaps 15,” Bujnowski called out, in the heat of the moment forgetting the correct setting for a go-around. Offchiss, knowing that flaps 15 was incorrect, set the flap lever to 25 degrees despite his captain’s order.
About five seconds after he called for the go-around, having yet to feel any response from the engines, Captain Bujnowski realized that he didn’t have enough time to get back in the air. On the verge of panic, he yanked the thrust levers back to idle and slammed on the brakes, sending the plane skidding down what remained of the runway with its nose still in the air.
Almost immediately, flight 625 hurtled past the end of the runway and onto the 150-meter paved overrun area.
“Oh shit!” someone shouted.
“Down!” Offchiss yelled. “Sta…!”
“Stop!” someone else screamed.
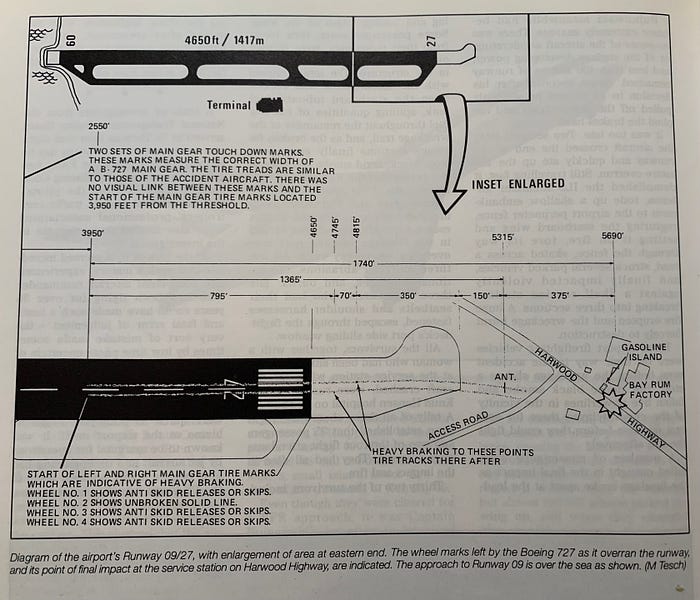
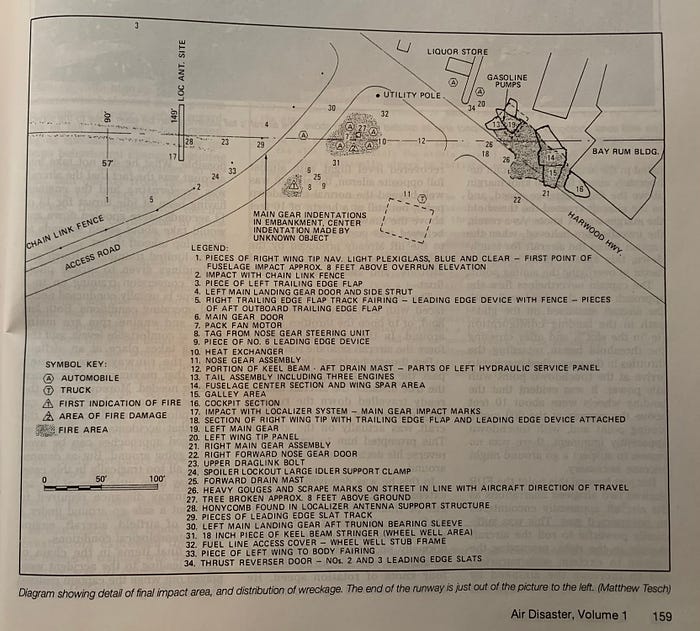
But it was already too late. Still traveling at about 80 knots, flight 625 left the paved surface and streaked across the grass, crushing the localizer antenna and slicing through a chain link fence. The right wing then slammed into an earthen embankment, sending the plane skidding sideways across the airport access road and onto the Harwood Highway (now Julian Jackson Drive), flames erupting in its wake as the ruptured right wing tanks ignited. Surrounded by fire, the 727 crushed several parked cars and knocked down a set of power lines before careening headlong into a Shell gas station, a rum factory, and the parking lot of a liquor store, where it finally lurched to a halt, broken into three pieces.
Although the breakup of the aircraft killed some people outright, the majority of those on board survived the initial impact, only to be faced with an immediate rush to escape as fire consumed the plane. Smoke and fire penetrated the cabin almost instantly, overwhelming passengers before they could even undo their seat belts. Someone managed to open the left overwing exits, providing an escape route into an alley, while others fled through breaks in the fuselage, some sustaining serious burns in the process. All three pilots were among the survivors, and despite their injuries they were able to flee the advancing flames through the first officer’s window. Two of the flight attendants also escaped, but two others did not, perishing in the inferno alongside 35 of their passengers.
By the time the first fire truck arrived on the scene two minutes after the crash, the evacuation was already over: everyone who would ultimately survive had already left the burning plane, which was now so completely consumed in smoke and fire that rescuers knew they would find no one to save. Although downed power lines and blowing smoke hindered the arrival of additional fire crews, there was nothing they could have done even if they had arrived sooner. Survivors later estimated that the entire evacuation lasted no more than 60 to 90 seconds; after that, conditions inside the plane became incompatible with human life. In all, during those 90 seconds, 51 people managed to escape with their lives, all but three of them having suffered some kind of injury, while 37 died in the crash and the fire which followed.

◊◊◊
The crash badly damaged several buildings, closed the island’s main road, injured a local resident who was waiting in their car, and generally confirmed Islanders’ and pilots’ worst fears about Harry S. Truman Airport. In an article on the accident, the New York Times cited air safety experts’ belief that such a crash was “almost bound to happen,” given the short runway’s limited margin for error. In fact, the airport was one of three in the United States which had been given a “black star” rating by the International Air Line Pilots Association due to its lack of infrastructure and hazardous surroundings. But all of this information, while important in a holistic sense, was not necessarily relevant to the proximate cause of the accident, which is what the National Transportation Safety Board was initially focused on finding.
Based on data from the 727’s primitive four-parameter flight data recorder, its cockpit voice recorder, and interviews with the pilots, the NTSB reconstructed a rough timeline of events aboard flight 625 with reference to the progress of the airplane along its final flight path. What they found was that everything was more or less normal as the plane approached the runway threshold, with a couple of notable exceptions.

For one, investigators felt that Captain Bujnowski should have extended the flaps to 40 degrees, not 30 degrees. The reason American Airlines wanted pilots to use 40 degrees of flap at St. Thomas was because the higher flap setting allowed the plane to land at a lower speed, reducing the required stopping distance. According to the 1971 bulletin, the captain could choose to land with flaps 30 if there were “strong, gusty winds,” and a later bulletin changed this to “strong OR gusty winds,” but the bulletins defined “strong” wind as any wind greater than 20 knots, while the actual wind was 10–12 knots, and there was no mention of gusts in the weather report given to the crew, so strictly speaking they should have used flaps 40, despite Bujnowski’s expectation that gusts would be encountered anyway.
The decision to use 30 degrees of flap played a small but subtle role in the events which followed. Specifically, using flaps 30 created less drag than flaps 40, which in turn made it harder to bleed off airspeed when Bujnowski attempted to slow the plane to plant it on the runway. He had already chosen an approach speed of 130 knots, 10 knots above the approach reference speed, and was traveling at 131 knots when he crossed the threshold. In order to get the plane to touch down, this speed needed to be reduced, and using flaps 40 would have made that easier. In the event, however, the plane was traveling several knots faster than optimal when it was struck by the sudden gust of wind which, as will soon be seen, led directly to the accident.

When a plane is about to touch down, it begins to experience “ground effect” — a natural increase in lift caused by the limited space between the wings and the ground. If a landing airplane already has too much lift, the introduction of ground effect can cause it to level off entirely, entering what is known as a “float,” in which the airplane skims along just above the runway surface without touching down. A float is more likely to occur at higher airspeeds or in the presence of strong headwinds. Flight 625 was already at increased risk of floating due to its high airspeed, but it probably would have touched down normally had a gust of wind not struck just as it reached the touchdown point, which lay about 330 meters (1,000 feet) down the 1,420-meter runway. The gust tilted the plane sharply to the right, occupying Bujnowski’s attention, while also causing a momentary increase in lift which, in combination with its high airspeed and the influence of ground effect, proved sufficient to trigger a float. The plane consequently leveled off at a height of 10 feet above the runway instead of touching down as the pilots probably expected.
Focused on his effort to prevent the right wing from striking the ground, Captain Bujnowski did not initially notice that the plane was floating. First Officer Offchiss called it to his attention four seconds later when he said, “Still high, Art.” Bujnowski reacted promptly, planting the wheels onto the runway two seconds after his first officer’s comment, but by then they were about 850 meters (2,800 feet) down the runway, well past the normal touchdown point. The danger of floating was thus made apparent, as the plane had used up a large portion of the 1,420-meter runway length during its 6-second float. Investigators noted that even without applying any brakes, deceleration is three to four times more effective when the wheels are touching the ground than when an airplane is floating.
At this point, there were only about 700 meters of paved surface remaining, including the 150-meter overrun area at the end of the runway. Captain Bujnowski therefore had to make a snap judgment: would this be enough room to bring his plane to a stop? In that moment, he decided that the answer was no, causing him to initiate a go-around three seconds after touchdown. Unfortunately, calculations performed by the NTSB and Boeing would prove that his snap judgment was wrong, a fact which also became apparent to Bujnowski himself about six seconds later.
Despite the fact that flight 625 had already traversed more than half the runway, the numbers showed that if Bujnowski had committed to landing, the plane probably would have stopped on the runway, and certainly would have stopped within the 150-meter paved overrun area. Had maximum braking been applied within two seconds, and maximum reverse within three seconds, the plane could have stopped in just 527 meters. On the other hand, despite Bujnowski’s inclination to abandon the landing when its success seemed to be in question, taking off again actually would have required more distance than stopping. Depending on whether Bujnowski moved the thrust levers in two stages or one, the go-around would have required an additional runway length of between 583 and 728 meters before the plane could become airborne. This would have surely resulted in a catastrophic crash, because by the time Bujnowski called out “Let’s go around,” there were only 515 meters of paved surface left including the overrun area. The NTSB also noted that in such a scenario, a pilot is likely to rotate for liftoff before achieving the required airspeed, resulting in increased drag which extends the takeoff distance even more.

The NTSB noted that despite his extensive experience, Captain Bujnowski might not necessarily have known that going around after touchdown could require more distance than stopping. In fact, the exact distance required to go around from a balked landing was not covered in training nor was it available in the operations manual. Furthermore, touch-and-go landings during training were typically conducted on long runways with a high engine power setting where the details of go-around performance were not a concern. These observations led investigators to a theory about why Bujnowski made the wrong decision.
Coincidentally, at the time Bujnowski decided to go around, flight 625 was still 150 meters short of the point at which he would normally rotate for liftoff while taking off from St. Thomas, and they were traveling at only two or three knots below the normal rotation speed. Therefore, Bujnowski might have looked at his position and instinctively noticed its resemblance to a normal takeoff at Harry S. Truman Airport, something he had accomplished many times before with a 100% success rate. Of course there was one key difference between a normal takeoff and the situation he was actually in, which was that flight 625 was decelerating with its engines at idle. When he made his snap judgment to take off again, Bujnowski did not consider that it would take between 6 and 9 seconds for the engines to spin up to takeoff power, during which time the plane would continue to use up more and more of the runway without reaching the conditions necessary for liftoff.
Bujnowski told investigators that he finally abandoned the go-around attempt when he did not feel or hear the acceleration he expected when he advanced the throttles. An examination of the engines showed that there was nothing wrong with any of them, but an analysis of the timeline revealed the problem: he simply hadn’t waited long enough. The time between his call to go around and his decision to cut the throttles and stop was only five seconds — not enough time for the engines to spin up to takeoff thrust. In fact, that was only enough time for them to reach an engine pressure ratio, or EPR, of 1.4, approximately half way between idle power and takeoff power. Not so coincidentally, this was the last EPR reading that First Officer Offchiss remembered seeing before Captain Bujnowski cut the throttles.

Bujnowski’s choice to reverse his earlier decision was the correct one, but by then a crash was already inevitable. Nevertheless, the NTSB found that Bujnowski could have significantly mitigated the outcome. In the event, he failed to push the nose wheel back onto the ground after the attempted go-around, and did not deploy the spoilers, resulting in a nose-high attitude which increased lift and reduced braking effectiveness. Furthermore, he did not apply reverse thrust until moments before the plane impacted the buildings. These two actions significantly impeded his ability to slow the airplane and likely increased the severity of the crash and the number of lives lost. NTSB investigators even stated that the plane might have stopped inside the airport perimeter had Bujnowski pushed the nose down and deployed the spoilers and reversers, although they did not cite any specific calculations to back up this assertion.
Bujnowski was not able to explain why he failed to take these measures, but the NTSB believed his actions to be consistent with the human panic response, which tends to impede reasoned decision-making by reverting to instinctive actions in an attempt to extract a person from danger as quickly as possible. In this case, detecting imminent disaster, his brain probably told him to slam on the wheel brakes as hard as possible, to the exclusion of all other concerns. The only way to overcome this panic response is to reprogram one’s instincts through rigorous repetition of training scenarios in which optimal use of all braking devices is necessary to ensure a safe outcome. At that time, however, no such training existed.

In the end, the NTSB identified two separate decisions by the captain which led to the accident: first, his decision not to go around immediately when the plane started to float, which was inconsistent with his training; and second, his decision to finally go around after it was already too late to do so. The float itself was caused by excessive airspeed on touchdown, in combination with an ill-timed gust of wind. In a later revision suggested by the Air Line Pilots Association, the NTSB also added the “non-availability of information about the aircraft’s go-around performance capabilities” as a contributing factor to the captain’s decision.
It is important, however, to take a step back and consider the situation in which Captain Bujnowski found himself. He was perhaps two seconds away from a completely normal touchdown when a gust of wind caught him off guard. The next thing he knew, the plane was floating, and his first officer was telling him he was too high. He instinctively put the plane on the ground, and then realized he’d landed long. Should he try to go around or should he try to stop? He didn’t know that this was a choice between life and death, as opposed to two benign outcomes, or two deadly ones — after all, what if there wasn’t enough room to go around or to stop? With 88 lives on the line, he had less than five seconds to decide, and he chose wrong. There is perhaps nothing more human than that.
A lot of thought has since been devoted to the question of why his high-stakes mental coin flip landed the way it did. In addition to the situation’s misleading resemblance to a normal takeoff, the NTSB suggested that foreshortening made the runway end appear closer than it actually was, causing him to prematurely rule out stopping as a safe course of action. Another idea was put forward by Stanley Roscoe in his book Aviation Psychology. Citing his own research as an aviation psychologist, he suggested that the cabin pressure anomaly earlier in the approach could have disturbed the interaction between the pilots’ vestibular and oculomotor systems, which has been shown to result in incorrect judgments about size and distance. In his opinion, Bujnowski might have misjudged both the nature of the float and the remaining runway distance because his eyesight was adversely affected by the lingering effects of the overpressure incident. But in the end, such decisions are often inscrutable even to those who make them, and the exact reason for the captain’s mistake will not and probably cannot ever be known. Conscious of this fact, American Airlines chose not to fire any of the pilots, and they resumed flying for the company after recovering from their injuries.

There was, of course, one more question: was Harry S. Truman Airport actually unsafe? Citing the fact that the crash was caused by human error and not the nature of the airport, the NTSB and the Federal Aviation Administration concluded that the answer was no. That conclusion received plenty of scrutiny at the time and deserves even more scrutiny today, on a philosophical as well as practical level.
The FAA originally approved operation of Boeing 727s into St. Thomas using the same criteria that it applied to any aircraft at any airport. American Airlines had proved that a 727 could lose an engine during a takeoff at maximum operating weight and still climb over the hills at the end of runway 9. It had also proved that a 727 could stop within 60% of the available paved surface without using reverse thrust after crossing the threshold at a height of 50 feet and on reference speed. These were the only limiting factors, and Harry S. Truman met both of them. Considering this fact, the NTSB wrote that “the airport, although less than ideal, is safe with regard to B-727–100 operations, provided that those operations are conducted within prescribed procedures.”

The caveat expressed in this quote is a highly important one. It carries within it an implicit assumption that any accident resulting from a deviation from prescribed procedures cannot reflect on the airport’s safety record. This was a common belief at the time, but it deserves to be questioned. In fact, Harry S. Truman Airport’s accident history was out of proportion with its traffic turnover levels. For example, in 1969, a Douglas DC-9 slid off the runway and collided with an auto repair shop, thankfully resulting in no fatalities. The accident was blamed on dynamic hydroplaning caused by excessive accumulation of water on the runway. Then in 1970, a Trans Caribbean Airways 727 crashed off the runway and burst into flames, killing two passengers, after the captain botched the recovery from a bounced landing. Now, in 1976, 37 people were dead because of a gust of wind and a captain’s split-second decision. By the NTSB’s logic, it would seem that only the first accident could be blamed on the airport directly. But when accidents continued to happen, involving different airlines and different pilots, it should have been apparent that the most obvious common denominator was the airport itself.

This is not to say that the airport “caused” the crash of flight 625, or the earlier Trans Caribbean crash. But what it did do was increase the latent level of risk on any given landing. That means that if a procedural deviation were to occur at St. Thomas, the potential consequences were greater than at other airports. As a result, St. Thomas could acquire a more extensive accident history than other airports with similar traffic turnover, even though each individual accident could be attributed to specific procedural deviations by the crew. By following this logic, an improper assumption becomes apparent in the NTSB’s argument concerning the safety of the airport: namely, that safety can only be measured against a theoretical distribution of outcomes which were possible while operating within the boundaries of prescribed procedures, even though actual operations took place outside those boundaries all the time.
This type of analysis requires subscribing to the rather modern notion that human errors are inherent in any system involving humans, and that the system itself should be constructed so as to mitigate the consequences of those errors whenever possible, even if parallel efforts exist to reduce the number of errors. In the case of Harry S. Truman Airport, we can therefore assert that the desired outcome — a lower rate of accidents — would best be achieved by increasing the length of the runway, reducing the risk of an overrun accident if a pilot misjudges a landing. Airlines could and did also try to provide better guidance to pilots to help them avoid the mistakes made by the crew of flight 625, but no such effort could ever be as effective as lengthening the runway, which would have prevented or mitigated all three of the aforementioned accidents on St. Thomas, regardless of what caused them.

In the end, it seems that someone with power did eventually see the light, as a runway expansion project broke ground in 1980 and was finished around 1984. The project involved filling in more of Brewers Bay, as well as removing several streets, a number of buildings, and an entire hill, eventually allowing the runway to reach its present length of 2,134 meters (7,000 feet). American Airlines, for its part, started routing its 727 flights to St. Croix, with smaller planes shuttling passengers to St. Thomas until the modifications were complete, at which point jet services resumed. Although attribution is tricky, it’s worth noting that to date, there hasn’t been another serious runway overrun accident at St. Thomas.
Even so, the non-exclusivity of human error and latent systemic risk factors is a topic which seemingly continues to confound certain people and organizations today. Arguments continue to be made, by entities such as Boeing, that the existence of pilot errors within an accident error chain somehow negates the responsibility of other parties to anticipate and mitigate such errors to the greatest extent possible. This type of thinking ignores the fact that no error ever occurs in a vacuum. Rather, pilots make decisions within an environment defined by risk factors that are sometimes outside their control. Captain Arthur Bujnowski had no influence over the length of the runway when he had to make his critical decision on April 27th, 1976. Arguments were no doubt advanced claiming that it was not the responsibility of the runway to bail him out when he made a mistake. On the other hand, if the runway had been extended earlier, 37 people might still be alive. And therein lies the lesson of flight 625: that the safety of the traveling public is best served by focusing not only on causes, but also on outcomes, regardless of who is to blame.
_________________________________________________________________
Join the discussion of this article on Reddit!
Visit r/admiralcloudberg to read and discuss over 220 similar articles.
You can also support me on Patreon.
