Margin of Error: The crash of Pacific Western Airlines flight 314
On the 11th of February 1978, a Pacific Western Boeing 737 on approach to Cranbrook, British Columbia crashed during an attempted go-around in the midst of a snow storm, killing 43 of the 49 people on board. But it soon became apparent that this was not a simple accident — somehow, on a lightly loaded flight to a small town in Canada, almost every conceivable type of error came together at exactly the wrong moment. Pacific Western flight 314 was brought down by a complex combination of air traffic control error, bad weather, flawed design, mechanical failure, and pilot error, comprising two entirely separate sequences of events that came to a head during a few critical seconds on the runway at Cranbrook Airport. More than 40 years later, the crash of flight 314 remains one of the most bizarre accidents in the history of commercial aviation — a testament to the principle that no air disaster ever has a single cause.

Founded in 1954, Pacific Western Airlines offered short haul flights to almost every town in western Canada for 33 years, linking isolated communities and mid-size towns that otherwise might not have received scheduled airline service. Amazingly, Pacific Western found this model to be quite profitable, and it expanded its routes with short range jets and turboprop airliners. Among them was the ubiquitous Boeing 737–200, the first mass-produced generation of Boeing’s most popular model.
One of these 737s began its day in Edmonton, Alberta on the 11th of February 1978. Early that morning, it began a long string of short hops, first flying to Fort McMurray, then back to Edmonton, and down to Calgary, from which it would continue to the British Columbian towns of Cranbrook and Castlegar. In command of the Calgary to Castlegar segments were Captain Chris Miles, age 30, an experienced pilot who had been flying since the age of 19; and First Officer Peter Van Oort, age 25, a new hire who had 82 hours on the 737. Shortly after noon, 44 passengers and 3 flight attendants joined the two pilots in boarding flight 314 to Cranbrook, totaling 49 occupants — barely a third of the plane’s capacity.
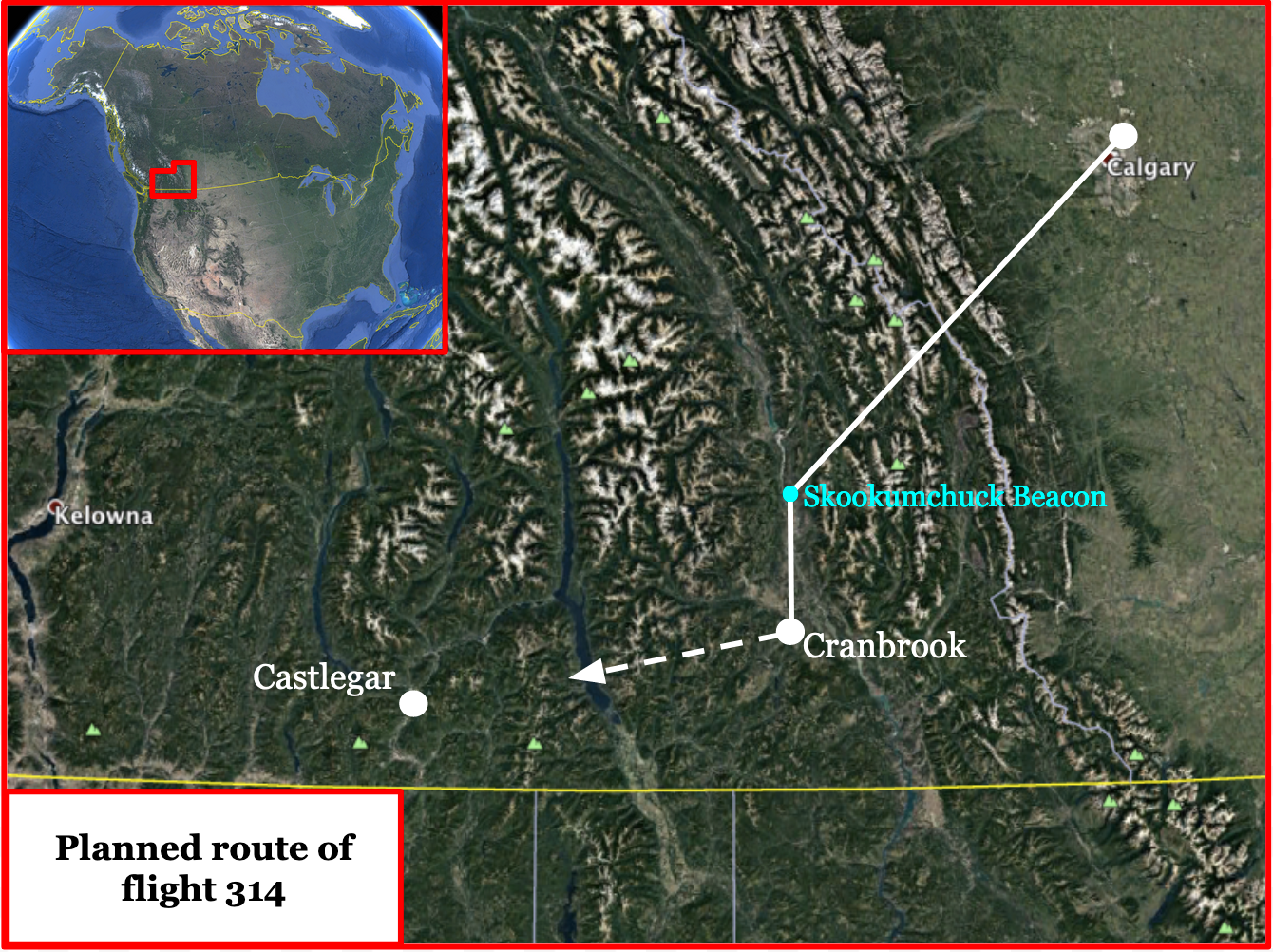
Despite ongoing snowfall in Cranbrook, Flight 314 took off from Calgary on time at 12:32 and headed west over the Rocky Mountains, its pilots expecting little difficulty despite the weather. At the moment of its departure, the air traffic controller in Calgary contacted his counterpart in Cranbrook and told him to expect flight 314 sometime around 1:05. This was a standard estimated time of arrival (ETA) that represented an outer limit — the latest the flight could be expected to arrive under normal conditions — and not a genuine attempt to predict its arrival time. Simultaneously, Pacific Western transmitted its own ETA to its baggage handlers in Cranbrook over a company channel. Unlike the ETA issued by the Calgary controller, this estimate came directly from the pilots, who figured they could get there 10 minutes earlier than the controller’s conservative figure.
Cranbrook was what is known as an uncontrolled airport. Due to a very light traffic load, it did not need an air traffic controller; instead, it had only an Aeradio operator, whose job was to give advisory information to pilots and to control ground vehicles within the airport. The Aeradio operator didn’t have the authority to give orders to pilots, who had full discretion regarding how they wanted to approach and land. It was this Aeradio operator who received the ETA of 1:05 from the air traffic controller in Calgary. At that time, up to a meter of snow had already fallen in Cranbrook and more was still coming down. In preparation for the incoming flight, the Aeradio operator sent out snowplow driver Terry George to clear the runway of snow. When Pacific Western flight 314 neared the airport, he planned to call George back off the runway.
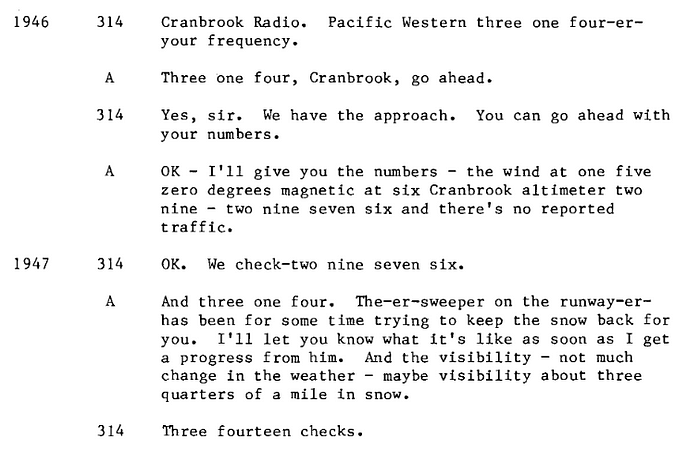
Meanwhile on board the 737, Captain Miles and First Officer Van Oort signed off with the Calgary controller, who cleared them to land in Cranbrook. First Officer Van Oort then contacted the Aeradio operator in Cranbrook and received a weather report — visibility was 1.2 kilometers in falling snow. The Aeradio operator added that a snowplow was out clearing the runway, and Van Oort replied, “Three fourteen checks.” This was the last communication between Cranbrook and flight 314.
Approaching the Skookumchuck beacon from the east, the pilots turned to the left to lock onto the ILS signal for a straight-in landing. It was customary for pilots approaching Cranbrook to report to the Aeradio operator when passing over the Skookumchuck beacon, but for reasons that remain unclear, the crew of flight 314 never checked in. It seems probable that they were distracted: after signing off with Calgary, First Officer Van Oort tuned in to the Cranbrook radio channel, but Captain Miles switched to a Pacific Western company frequency that was not related to flight operations. Since he was flying the plane, he should have been listening to the Cranbrook frequency, not engaging in off-topic discussions with other PWA employees. Most likely, with Captain Miles distracted, the duty of informing the Aeradio operator of the plane’s position fell to the inexperienced first officer, who simply forgot to do so.
The stage was now set for a problem: the pilots of flight 314, although aware of the snowplow on the runway, likely assumed that it would be called off before they arrived at 12:55. However, the Aeradio operator hadn’t received an update on the plane’s position and still assumed it would arrive at 1:05. Unaware that the 737 was moments from landing, he never called Terry George and his snowplow back to base.
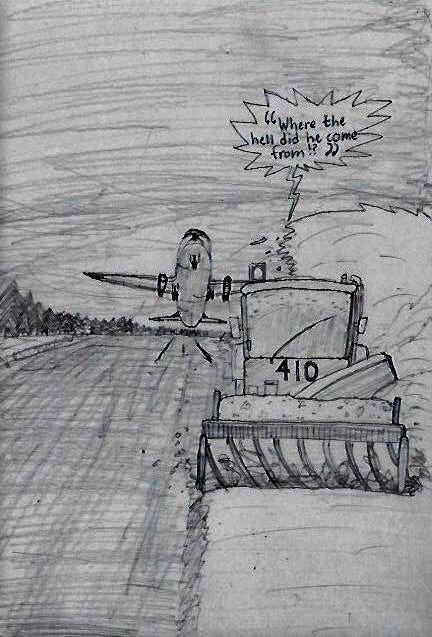
At 12:55, flight 314 arrived at Cranbrook Airport with no warning whatsoever. On board the 737, the pilots were initially unable to see the snowplow because it threw up a plume of snow that obscured it against a featureless white background. Captain Miles brought the plane down on the runway, rolled the engines back to idle power, and started to apply reverse thrust to slow the plane. But barely two seconds after touchdown, he suddenly caught sight of the snowplow, which was still on the runway. At that exact moment, George looked back from the cab of his snowplow to see a large passenger jet touching down just 300 meters behind him!
There was no time for the pilots to debate what to do. Miles knew that he had only seconds to prevent a potentially catastrophic collision with the snowplow, and he took action immediately. With incredible speed, he called for a go-around, cancelled the reverse thrust command, slammed the throttles to max power, and pulled back to climb. Simultaneously, George made a last-ditch attempt to steer his unwieldy snowplow out of the way, but there was nowhere to run. Over the ground radio frequency, he shouted, “Where the hell did he come from?”
On the 737, Captain Miles had inadvertently discovered a loophole in the protections built in to the jet’s thrust reverser system. Early 737s had “bucket-style” reversers, where hydraulically-actuated doors folded down over the engine exhaust channel to redirect thrust forward. The hydraulic actuators require several seconds to fully open or close the doors, during which time the application of greater than idle thrust is inhibited via an interlock system. When Captain Miles canceled the reverse thrust, the partially open reverser doors started moving back toward the closed position. But due to the mechanical design of the reverser interlock system, it was possible to begin applying full forward thrust when the reverser doors were almost closed rather than fully closed. Miles initiated the go-around so quickly that he managed to accelerate the engines to max power and lift off the ground before the hydraulic actuators had quite finished closing the bucket doors on the left thrust reverser.

To prevent deployment of a thrust reverser in flight, an isolation valve cuts off hydraulic fluid from the reverser actuator unless the main landing gear is touching the ground, the engine is running, and the engine is not on fire. If any of these conditions are not met, the valve closes, and the actuator cannot move the reverser doors. As flight 314 lifted off the runway during its last second go-around, the plane’s weight was removed from the landing gear, and the hydraulic isolation valve closed, cutting off power to the left thrust reverser actuator. But at that moment, the left reverser doors were 5 centimeters short of fully closed — in fact, the isolation valve, which was meant to lock the reverser shut, had instead locked it in the partially open position!
At the moment of liftoff, the cockpit of flight 314 plunged into chaos. Miles and Van Oort had together pushed so hard on the throttle levers that Miles fractured his thumb, probably causing intense pain. Their plane was also still configured to land, not to climb: the landing gear was down and the flaps were still extended, causing significant drag. Still, the 737 managed to clear the snowplow by just a few meters, its landing gear passing right over George’s head as he cowered in terror.
As the plane picked up speed, aerodynamic forces pushing into the gap formed by the partially open left thrust reverser doors wrenched the reverser back to the fully deployed position. Sensing a mismatch between the positions of the reverser and the throttle lever, a safety system automatically reduced thrust on the left engine to idle to prevent it from generating full reverse power in midair. But now flight 314 was trying to climb in a high-drag configuration with its right engine at climb thrust and its left engine in idle reverse. The plane yawed to the left, and the pilots instinctively countered with right rudder and aileron inputs, but they quickly started losing speed. Realizing that the left reverser had deployed, First Officer Van Oort apparently recalled that hydraulic power could be restored to the reverser using the reverser override switch, which would allow them to close it. The switch, located above and behind the first officer, is intended for maintenance use but can be activated in flight in the event of an emergency. Evidence indicates that Van Oort retracted the flaps and then stood up in his seat in a desperate attempt to reach the reverser override switch. But as he did so, one of the pilots accidentally let off the pressure on the right rudder pedal, causing the plane to roll sharply to the left again. Van Oort managed to open the safety case covering the override switch, breaking its witness wire, but was thrown off balance before he could flip the switch itself.
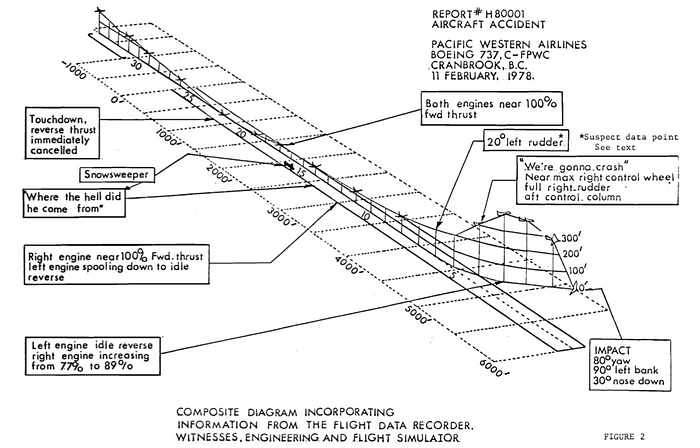
At that point, the plane was nigh unflyable. It had decelerated dangerously and yawed to the left, which reduced its speed even further. It was the low speed that finally did them in: as speed decreases, so does the effectiveness of the flight controls, which rely on a fast-moving airstream. Less than 10 seconds into the go-around, flight 314 decelerated to the point that the rudder and ailerons were no longer sufficiently powerful to overcome the plane’s desire to pull to the left. The 737 rapidly rolled into a 90-degree left bank, stalled, and plunged from the sky at an altitude of barely 400 feet. Passengers hung on in terrified silence as the plane tilted sideways, granting its occupants a clear view of the rapidly approaching ground. Over the radio, Captain Miles could be heard screaming, “We’re gonna craaaaash!”

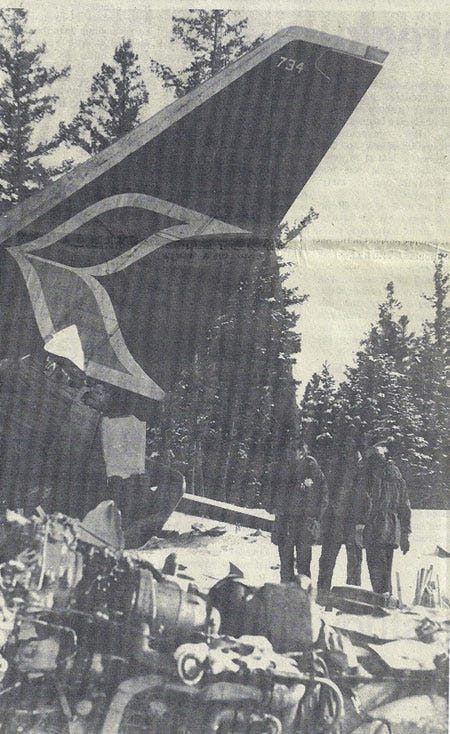
Moments later, flight 314 plowed into a snow-covered field off the left side of the runway. The cockpit and left wing struck the ground first, igniting a fireball as the fuel tanks burst open. The fuselage crumpled like an accordion and disintegrated, throwing passengers out into the fire and snow, many of them still strapped into their seats. The tail section continued forward, crushing the center of the cabin before coming to rest alongside mangled remains of the cockpit.

At the very back of the plane, flight attendant Gail Dunn was stunned to discover that she had survived the crash essentially unharmed. So had a young man sitting in the last row, who rushed back to help her open the emergency exit door. The two survivors stumbled out of the burning plane and into knee-deep snow, where they were confronted with a scene of total carnage. Wreckage and bodies lay strewn about the field, and a huge fire was consuming the remains of the passenger cabin. Just outside the plane they managed to find an 11-year-old girl lying in the snow, injured but alive; as they dragged her away from the flames, she screamed for them to return for her mother, but the fire was too intense and they were beaten back.

Meanwhile in the Aeradio office, the Calgary controller called the operator and reported, “Cranbrook radio, Calgary. I’ve got an inbound for you.”
“Standby a second please, I got an emergency,” the operator replied. At that moment, Terry George and the airport’s two firefighters jumped into their sole emergency vehicle and rushed to the scene of the crash. Finding their path blocked by deep snow, they abandoned the truck and continued forward on foot, arriving on the scene just a few minutes after the accident. Amid the burning the wreckage, they found several more survivors, one of whom had been sitting just behind the wings and was ejected during the breakup. Two others seated in the intact tail section had escaped through the break in the fuselage and were found wandering in the snow. Including the two who went out the emergency exit and the young girl they saved, the initial rescue effort turned up six survivors, all but one of whom had been sitting in the last four rows. Inside the remains of the forward cabin, the firefighters managed to find a seventh survivor clinging to life despite a severe head injury.
Nine minutes after the crash, Calgary ATC called the Cranbrook Aeradio operator again. “Cranbrook radio, Calgary, are you still busy?”
“Ah, okay, go ahead now Calgary.”
“Okay, first off, where’s PW three fourteen now, have you any idea?” the controller asked.
“Yeah, he’s the emergency,” the operator replied. “He’s crashed and is burning off the end of the runway.”
Cranbrook Airport is located 10 kilometers outside the town itself, and it took 25 minutes for firefighters to arrive from the communities of Cranbrook and Kimberley. By the time they reached the scene, the fire had consumed most of the plane, and the heroic airport employees had already managed to extract all the survivors they could. It took a further hour and a half for a snow blower to clear a path for the fire trucks to approach the wreckage, where they finally managed to put out the blaze and started the long, grim recovery process.
Eleven days after the crash, the survivor extracted from the front of the plane died in hospital, bringing the final death toll to 43 with six survivors. In a small town like Cranbrook, the crash dealt a massive blow to the local community. Most residents knew one or more victims (as did one of the responding firefighters, whose father was on the plane). Some of the passengers had intended to continue on to Castlegar, and that community was affected as well. Numerous children lost parents, including some who needed decades to get their lives back on track.

Investigators from Transport Canada trying to uncover the cause faced an immediate setback: due to its prolonged exposure to fire, the cockpit voice recorder had been destroyed, and the flight data recorder suffered damage that rendered some of its parameters unreadable. In the absence of some of the most definitive sources of evidence, numerous parties tried to push their own narratives. Initially, many in Cranbrook blamed snowplow operator Terry George, but it was soon clear that he had nothing to do with the crash — in fact, he was one of the story’s heroes, running to join the firefighters on their rescue mission before he’d even had time to recover from his near-death experience. A longer court battle then ensued over who was really to blame for the accident: was it Transport Canada? The pilots? Boeing? The answer, according to the final report, turned out to be all three.
The full story of the crash had to be split up into two main error chains: the miscommunications that put flight 314 in conflict with the snowplow, and the mechanical and human errors that led to a loss of control during the go-around. Regarding the former, investigators pointed to a lack of airmanship on the part of the pilots, as well as insufficient regulations. There were no rules governing how ETAs should be used, and only vague rules about how they should be created. The Aeradio operator used Calgary’s ETA to determine when it was safe for ground vehicles to occupy the runway, a dangerous practice that made a near miss, if not an accident, inevitable from the beginning. In fact, Calgary’s ETAs for the Calgary-Cranbrook route were in error by an average of five minutes, with some off by as much as 13 minutes, despite the fact that a flight involving a straight-in approach to Cranbrook almost always took 25 minutes with little variation. Both the controller and the Aeradio operator displayed poor handling of the situation leading up to the accident.
The pilots also played a role in the miscommunication. Regulations did not technically require that pilots inform an Aeradio operator that they are approaching the airport, but pilots interviewed during the investigation agreed that a failure to do so would be poor airmanship. Calling in over the Skookumchuck beacon was therefore customary but not legally obligatory. Transport Canada investigators felt that if it had been a written requirement, the pilots might not have forgotten it (although the exact reason why they didn’t call in could not be determined). Contributing to the problem was the fact that the position of “Aeradio operator” was barely mentioned in Canadian air traffic control regulations and had no clearly defined duties, resulting in considerable variance in the level of interaction pilots could expect from operators at different uncontrolled airports.

Investigators also found that in 1977, Boeing updated the relevant section of its 737 flight manual to read, “Do not attempt a go-around after reverse thrust has been initiated. Failure of a thrust reverser to return to the forward thrust position may prevent a successful go-around.” Clearly this concern was well-founded, as it warned of the exact failure scenario that brought down flight 314. But the update, added only months before the crash, came well after Captain Miles went through training. Furthermore, investigators identified several other incidents — some of them involving Pacific Western — in which crews executed successful go-arounds after application of reverse thrust. These might have lulled Miles into a false sense of security, obscuring the fact that Boeing believed such a move to be dangerous.
However, Transport Canada felt that if canceling reverse thrust for a late go-around was dangerous, then something must be wrong with the design. “It is accepted that the 737 thrust reverser design was in compliance with the applicable FAA standards under which the aircraft was constructed,” they wrote. “[But] considering that the aircraft was intended for use at smaller, ‘uncontrolled’ airports, as well as at main line airports, the ability to abort a landing even after touchdown and reverse selection would seem to be a desirable, if not essential, feature. In this sense the FAA standards must be considered either inadequate or ill-defined.” It was therefore hard to ding the pilots for attempting a dangerous procedure that should never have been dangerous in the first place. Given that Captain Miles had only two or three seconds to decide whether to perform a late go-around or crash into the snowplow with potentially catastrophic results, his decision to cancel reverse thrust was understandable.

Transport Canada further criticized the reverser design over the loophole that allowed it to deploy in flight. Tests showed that if the isolation valve closed while the reverser doors were more than a couple centimeters open, they would invariably deploy again as the plane picked up speed. The logic of the interlock system could in fact be used to cause the exact failure it was supposed to prevent. Although the reverser design met regulatory requirements as they stood when the plane was certified in 1967, Transport Canada expressed skepticism that the design would pass muster if recertified in 1978. It certainly would not work today: in addition to the fact that most aircraft no longer use bucket doors that could be deployed by aerodynamic forces, typical modern thrust reverser interlock systems continuously energize the “stow” circuit so that unless the reversers are specifically commanded to open, they will always return to the fully closed position. Due to these changes, it would be impossible for a modern reverser to fail in the same manner.

Despite the deployment of the reverser, tests showed that flight 314 would have been controllable had Miles and Van Oort consistently maintained full right aileron and rudder throughout the climb. However, the pilots faced an extremely heavy workload in the 20 seconds between the initiation of the go-around and the crash. Not only did Captain Miles face the simultaneous shock of an encounter with a snowplow and an uncommanded reverser deployment, he is also thought to have fractured his thumb while moving the throttle levers to max power. He would have had so much on his mind in those first critical seconds that he was bound to miss something. The failure to retract the landing gear and flaps was therefore understandable, even though it put the plane into an extremely precarious situation. All it took to throw the flight permanently off balance was a momentary cessation of the right rudder input. While it’s unclear exactly why this occurred, investigators speculated that it might have been the result of First Officer Van Oort standing up to reach for the reverser override switch; Captain Miles involuntarily reacting to the pain of his fractured thumb; or a combination of both. During a civil suit over the crash, Boeing pointed to a large left rudder input on the flight data recorder as evidence that the pilots caused the loss of control; however, Transport Canada ultimately concluded that this reading was false, because if it had occurred as recorded, the plane would have crashed sooner than it actually did.

Today, tougher regulations address the causes of the crash on every level. There are standards for the creation and use of ETAs; a clearly defined role for radio operators at uncontrolled airports; a legal requirement for pilots to inform the radio operator when approaching an airport; and much wider use of radar, especially at mountainous airports. Although procedures today clarify the fact that a go-around should not be performed after application of reverse thrust, if one were to be attempted anyway, modern reversers ensure that the chances of an inadvertent deployment are much lower. In fact, the reverser design on 1960s-era Pratt & Whitney JT8D engines like those on the 737–200 would fail to meet modern certification requirements in several areas, which illustrates just how far safety has progressed on a systemic level since the 737 was first introduced. Canada also introduced a unique requirement stipulating that all new airplanes certified there must be able to perform a so-called “Cranbrook maneuver” without the engines becoming stuck in reverse thrust.
The crash of Pacific Western flight 314 stands out today not necessarily because of its safety impact, but because it shows just how complex the causes of air disasters can be. So many people made so many errors — the controller, the Aeradio operator, the pilots, Boeing, Canadian regulators — that it becomes obvious why no one person is to blame. If any of these people or organizations had done one small thing differently, the accident wouldn’t have happened. What if the pilots had reported their position? What if the controller had issued a more accurate ETA? What if Boeing had designed a thrust reverser interlock system that didn’t allow max thrust to be applied until the reverser doors were completely closed? And, of course, none of these errors would have mattered if not for the bad weather, the random chance factor that ultimately decides whether a series of mistakes ends in tragedy. And it also reminds us that even in 1978, it took a lot to bring down a plane. Even after everything that went wrong — the encounter with the snowplow, the go-around, the reverser deployment, the incorrect aircraft configuration — the plane would have been just barely flyable if the pilots had managed to keep their feet firmly on the rudder pedals. Sadly, in the chaos that gripped the cockpit, it is understandable (if still regrettable) that they did not. For the families of the 43 who died, and for the six survivors who must live with the injuries they received, the question of what could have been done differently will forever linger in the back of their minds.
______________________________________________________________
Click here to join the discussion of this article on Reddit!
And don’t forget to visit r/admiralcloudberg for over 100 similar articles.
