Overworked and Underpaid: The crash of TransAsia Airways flight 222

On the 23rd of July 2014, a regional flight approaching an island off the coast of Taiwan suddenly slammed into a village short of the airport, demolishing nine houses and killing 48 of the 58 passengers and crew. At first, many speculated that Taiwan’s first major crash in 12 years might have had something to do with the outer bands of a typhoon which were strafing the airport at the time of the accident. But investigators would find that bad weather was only a small part of a story involving a tired captain, a lack of respect for standard procedures, and poor cockpit communication — a milieu of factors which had led to countless crashes in earlier decades. That a crew in 2014 would make these mistakes raised red flags about the rapidly expanding carrier, TransAsia Airways. Seeking to understand the context in which the crash occurred, Taiwan’s Aviation Safety Council dived deeper, revealing how the airline sidelined safety in the pursuit of growth, and how the Civil Aviation Authority missed dire warning signs. But amid the controversy surrounding who was at fault, TransAsia Airways continued full steam ahead — until another crash, and another 43 deaths, finally forced authorities to confront the problem.
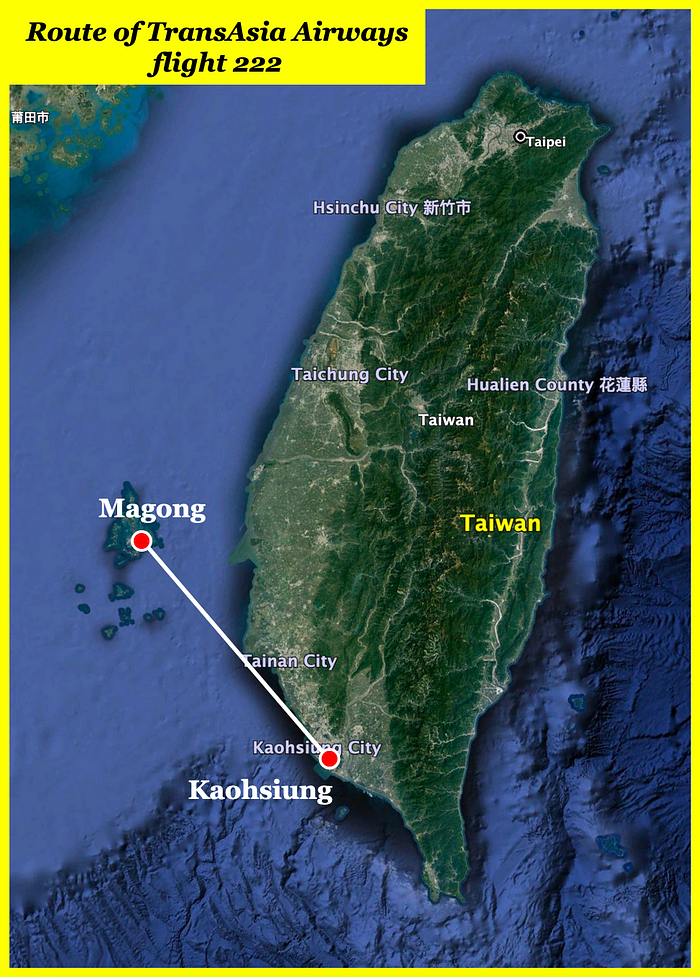
Fifty kilometers off the west coast of Taiwan lie the Penghu Islands, a ragged archipelago made up of 90 small islets which are collectively home to about 100,000 people. Historically known for both their fishing and drug trafficking industries, the islands are increasingly popular with tourists, who, like many locals, fly frequently on short hops across the strait from cities in western Taiwan. In 2014, the cheapest and most convenient option for travelers to the Penghu Islands was TransAsia Airways, a fast-growing regional airline specializing in domestic flights within Taiwan.
Founded in 1951 as Foshing Airways, TransAsia was the first privately owned airline in Taiwan, but from 1958 to 1988 it became exclusively a travel agency and did not operate any aircraft. After returning to the airline market, now freshly rebranded as TransAsia Airways, it formed a core domestic fleet consisting of several ATR-72 regional turboprops, from which it leapt quickly into international jet services, acquiring a large number of wide- and narrow-body Airbus aircraft. The airline’s growth accelerated further in the early 2010s, becoming a publicly traded company in 2011, launching a subsidiary, and rapidly expanding its fleet. But, like a corporate Icarus, TransAsia would ultimately fly too close to the sun in its relentless pursuit of financial success.

◊◊◊
The 23rd of July 2014 was a regular day on the job for 60-year-old TransAsia Captain Lee Yi-liang and his 39-year-old rookie First Officer Chiang Kuan-hsing. Lee, who had been flying the ATR-72 since 1992 and had 19,000 hours on the type, and Chiang, a new hire who started flying in 2011, had been hopping around Taiwan together for several days. Yesterday they completed no less than seven flights, and today they were scheduled for another six. By evening, they had already flown from Kaohsiung to Magong, the main city in the Penghu Islands, then back to Kaohsiung. Like a shuttle service, the pilots and their plane now prepared to return to Magong for the second time that day, and the tenth time that week.
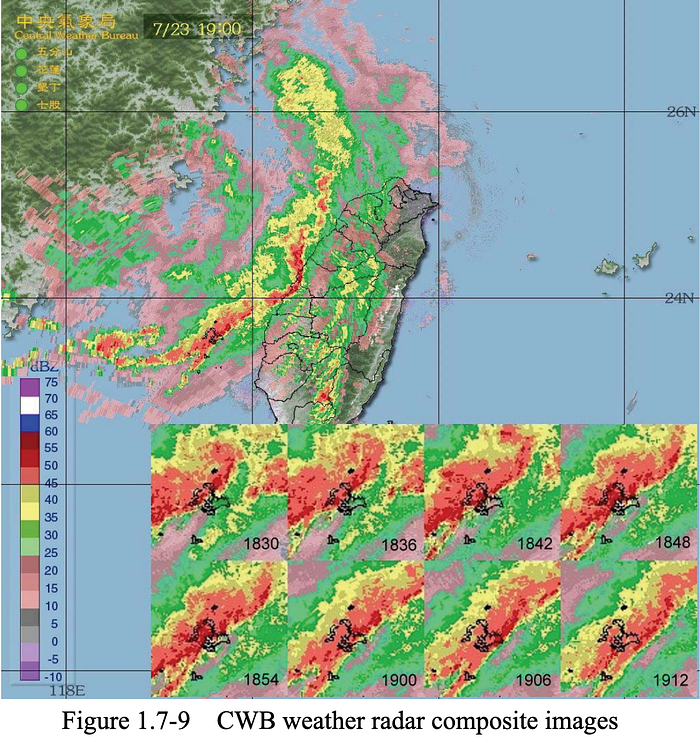
With 54 passengers and four crewmembers on board, TransAsia Airways flight 222 departed Kaohsiung at 17:45 local time for what should have been a brief, 45-minute flight to Magong. But the pilots already knew to expect delays: earlier that day, Typhoon Matmo had grazed the Penghu Islands as it churned north up the Taiwan Strait, and the cyclone’s outer thunderstorm bands were still rolling across the archipelago, one after another.
From the very beginning, Captain Lee seemed under the weather. The cockpit voice recorder captured him alternately yawning and coughing for minutes on end, and at 18:10 he said “Aaah, I’m so [damn] tired,” eliciting no particular comment from First Officer Chiang.
At that time, the weather was unsuitable for landing at Magong Airport. The default landing option was runway 02, which was equipped with an instrument landing system to help crews in conditions of low visibility; but tonight it could not be used because it was subject to a strong tailwind. At the same time, the opposite runway 20, which had a favorable headwind, lacked an instrument landing system and as such could not be used if the visibility was below 1,600 meters. By the time flight 222 arrived in the region, the visibility was only 800 meters, well short of the minimum, preventing landing on this runway as well. Therefore flight 222 was placed into a holding pattern north of the airport, along with three other aircraft, in order to wait for conditions to improve.
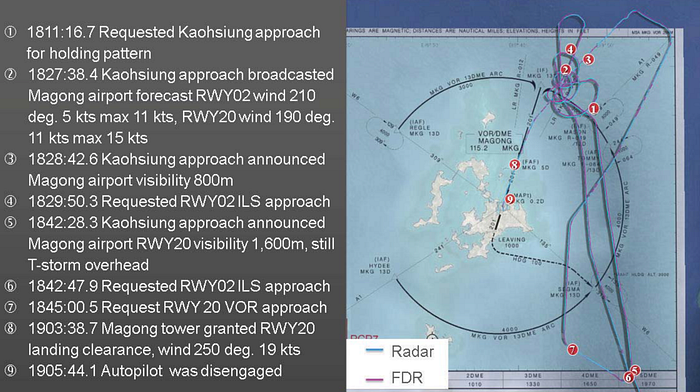
At 18:29, after holding for 18 minutes, the pilots heard in a routine weather report that the tailwind on runway 02 had decreased to only 5 knots, well within limits. Jumping on the chance to land, they requested permission from air traffic control to join the approach pattern for runway 02, as did a Uni Air flight ahead of them. But at Magong Airport, which is jointly run by the civilian airport authority and the Taiwanese military, the controller had to coordinate with his Air Force counterpart before he could change the runway in use, which up until then had been runway 20. This promised to take quite some time, and so flight 222 kept circling in the hold, waiting for permission to land.
Instead, at 18:42, a weather report revealed that the visibility at the airport had increased to 1,600 meters, the minimum required for landing on runway 20. The pilots seized on this report as an opportunity to land without delay, and requested permission to return to their original plan to come straight in to the south and land on runway 20. It worked: the controller immediately cleared them to a lower altitude and vectored them toward the approach pattern, and at 18:55 they were cleared to begin the approach.
Flight 222 was flying what is known as a VOR approach. This is a non-precision approach, meaning that ground-based equipment does not guide the crew in both the vertical and lateral planes. In a VOR approach, the crew tracks a specific radial of a VOR radio beacon located at the airport, allowing them to line up with the runway quite precisely, but without any altitude guidance. Instead, pilots calculate and select a descent rate and angle which will bring them to within sight of the runway at the proper altitude.
On this particular approach, they were not allowed to descend below a minimum descent altitude (MDA) of 330 feet unless they could see the runway. Upon reaching this altitude, they were required to level off, but could continue to fly level until reaching the designated missed approach point located two kilometers from the runway threshold, at which point they were obligated to abandon the approach if the runway was still not visible.
Having flown to Magong dozens of times, the pilots were already quite familiar with the VOR approach to runway 20, and they knew most of the numbers by heart. Captain Lee, apparently confident in his understanding of the procedure, never called for the mandatory approach briefing, nor did the crew conduct the descent/approach checklist, during which they would cross-check their course, speed, and other settings. Instead, Captain Lee simply ordered First Officer Chiang to select a target altitude of 400 feet in the autopilot control panel.
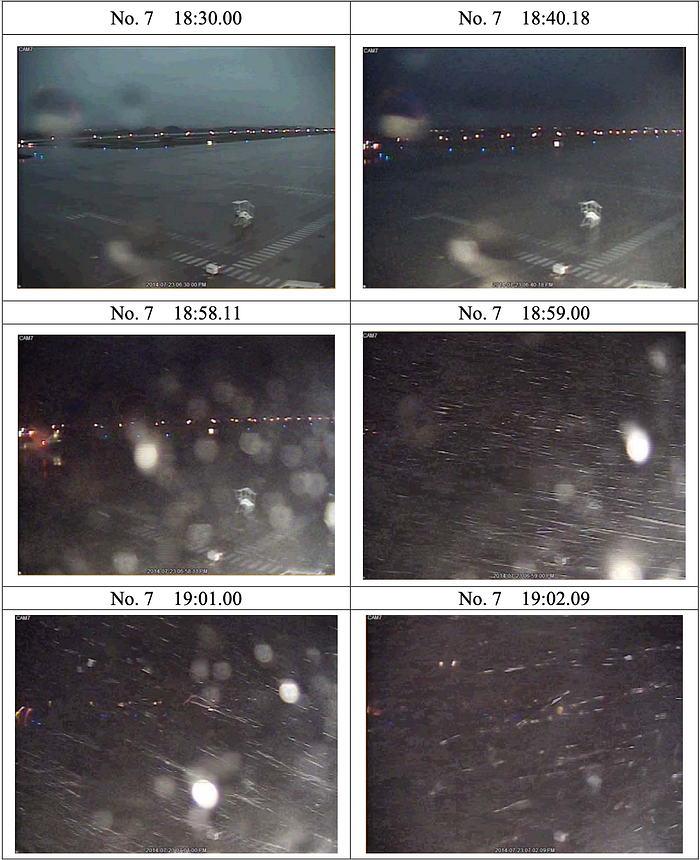
At about 19:01, as flight 222 descended on final approach, the next band of thunderstorms suddenly slammed into Magong Airport. The pilots of the Uni Air flight, which had just touched down and was taxiing to the parking area, found themselves pounded by a torrential downpour which seemingly came out of nowhere. So heavy was the rain that they elected not to disembark the passengers until the squall had passed.
In the control tower, automatic visibility range readings over the runway plunged from 1,600 meters to less than 800, way below the minimum for landing on runway 20. The controller, however, mistrusted the automatic measuring system because it sometimes differed significantly from the measurements made by human weather observers. As the storm moved over the airport, a new broadcast went out from the Magong Airport meteorological office indicating that the observed visibility was still 1,600 meters. The controller on duty called his supervisor to ask which reading he should use, and the supervisor told him to trust the human weather observer over the automated sensor. And so the system continued to display the runway visibility range — 650 meters, then 550, then 450 — but the controller never informed the crew of TransAsia Airways flight 222.
Descending through 500 feet, flight 222 entered the storm, and the cockpit voice recorder picked up the sound of heavy rain drumming on the windscreen.
“FIVE HUNDRED,” an automated voice announced.
“Um, three hundred,” Captain Lee said, instructing First Officer Chiang to select a new target altitude of 300 feet. Chiang immediately reached over and inputted the new value.
For another few seconds, the plane kept descending. There was still no sign of the runway. Captain Lee yawned loudly.
The plane reached the MDA of 330 feet. Still nothing. With a tired sigh, Captain Lee said, “Two hundred.”
It would be a serious violation of standard procedures to descend below the MDA without the runway in sight, but no one objected. First Officer Chiang dutifully entered 200 feet into the autopilot.
Seconds later, as the plane passed through 219 feet, Captain Lee disengaged the autopilot and announced, “Okay, maintain two hundred.” He pulled back to level off, and the plane pulled out of its descent just below 200 feet.
After nine seconds, Lee asked, “Have you seen the runway?”
“Runway?”
“Um,” Lee said, staring out into the driving rain. The visibility was shockingly bad. “Wow,” he muttered, letting out a little nervous laughter.
After staring out the window for some time, Chiang announced, “No.”
“No?”
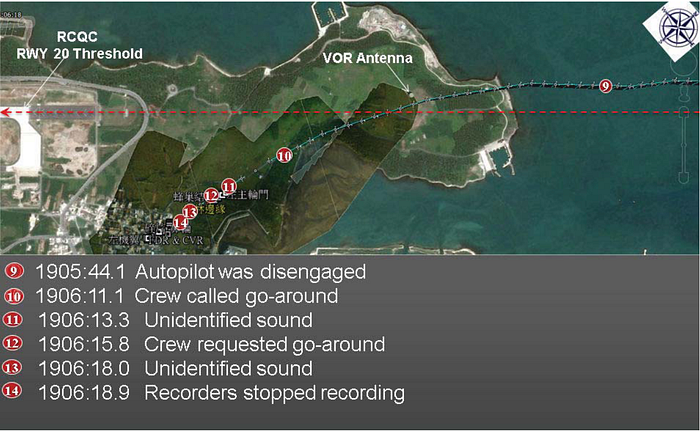
“No sir,” Chiang repeated. The runway could not be seen through the swirling storm. At this point the plane reached and then passed the missed approach point, where they were supposed to go around if they had not sighted the runway. But they kept going.
The pilots had now spent thirteen seconds staring into the blackness trying to spot the runway, but during those thirteen seconds the plane started to drift off course. Subtle inputs on the captain’s control column pushed the nose down and steered the plane to the left, causing it to slowly descend toward the ground to the left of the approach path. Neither pilot knew it, but they were only seconds from impact.
As it became clear that they would not be able to see the runway, Captain Lee said, “Okay, okay, okay,” seemingly preparing to abandon the approach.
Less than one second later, First Officer Chiang must have seen that they were dangerously low, or perhaps he spotted objects looming up ahead of them, because he suddenly shouted, “Go around!”
“Go around!” Lee exclaimed at almost the exact same moment. But it was already too late. As Lee reached for the throttle levers, the plane began to strike trees, branches and trunks tearing at the wings and fuselage.
Chiang keyed his mic and managed to say to the tower, “Go around, go around!”
“Roger,” the controller said. He began to ask to where flight 222 planned to climb, but he would never receive a reply.
Badly damaged from the tree strike, the ATR-72 emerged from the forest, cleared a field, and slammed headlong into the edge of Xixi village, a community located about 850 meters northeast of the runway threshold. The right wing struck a two-story building and the plane spun around nearly 180 degrees, splitting in two as it slammed down on top of several houses. Amid a wave of flying masonry and burning fuel, the mangled wreckage rolled to a halt across an alleyway, its busted seats and shattered windows lying open beneath the rain.
Remarkably, some of those on board managed to survive the violent impact. Several were thrown from the plane as it was still in motion, coming to their senses lying on the ground nearby; others awoke inside the twisted remains of the burning fuselage and managed to crawl to safety. As residents of the village hurried to help, the survivors gathered in a nearby house to wait for emergency services. One passenger immediately called her father to report that she had survived — ironically, he would be one of the first to hear about the accident.
Emergency crews soon arrived and rushed the survivors to hospital, where they all made a full recovery, despite serious injuries. Five people in the village were also injured, but no one the ground was killed, an outcome which could only be considered miraculous, given that no less than nine buildings were destroyed when the ATR-72 plowed into the town. Unfortunately, those on board the plane were not so lucky: in all, 48 people lay dead, including all the crewmembers.

The crash of TransAsia Airways flight 222 was the first major plane crash in Taiwan since 2002, and the first loss of a passenger flight in the airline’s history. Appearing before the media, the president of TransAsia tearfully apologized to the families of the victims, while authorities vowed an impartial inquiry.
Responsibility for the investigation would fall to the Aviation Safety Council of Taiwan (ASC), which sent investigators to Penghu the following day. Meanwhile, the black boxes were flown to Taipei, where investigators were able to listen to the pilots’ conversations before and during the ill-fated flight. What they found was a story of an accident that had already happened many times before.

The basic cause of the accident was the captain’s decision to descend below the minimum descent altitude without being able to see the runway, a decision which has led to the lion’s share of controlled flight into terrain accidents throughout history. Flying too close to the ground, Captain Lee didn’t leave himself with a large enough margin for error, and so when he became distracted and let the plane drift downward for a mere 13 seconds, disaster became unavoidable. The lack of proper control over the flight path in the last moments of the flight was sloppy, but it only resulted in a crash because the plane was too low to begin with. That’s why the MDA lies well above the terrain — to ensure a sufficient safety margin even if the crew makes other errors. By violating it, Captain Lee put himself in a position where he needed to fly perfectly in order to avoid an accident, but he did not do so.

Furthermore, First Officer Chiang did not challenge Captain Lee’s decision, even though it violated one of aviation’s most fundamental safety rules. Instead, when Lee asked him to enter an altitude of 200 feet into the autopilot, he complied without question. Investigators noted that a steep authority gradient likely existed between the 60-year-old captain, who had 22,000 flight hours, and the much younger First Officer, who had only about 2,000. Nevertheless, the problem of submissive first officers failing to question senior captains should have been solved long ago with the introduction of crew resource management training, which taught first officers how to speak up about their concerns and trained captains to accept their input. The fact that such a basic problem had cropped up in yet another accident, in 2014, raised questions about the quality of training at the airline. This was not the 1970s — the industry already knew the solutions to these problems.

The black boxes further revealed that the crew had been sloppy throughout the flight, not just in its final moments. The pilots skipped checklists, missed important callouts, and failed to conduct an approach briefing, among two dozen or so errors ultimately noticed by investigators. The sheer number of procedural errors raised another red flag. How exactly were TransAsia pilots flying their planes, day in and day out?
When the ASC sent investigators to ride aboard a number of routine TransAsia flights, they were stunned to find widespread disregard for standard procedures. Pilots were fast and loose with their checklists, executing some from memory and skipping others altogether. Required callouts of altitude, autopilot mode, and many other parameters were routinely ignored. Several pilots flew too low on approach or descended too quickly without eliciting any comment from the monitoring pilot. It didn’t take long to conclude that something was seriously amiss.
A culture of disregard for standard procedures can only arise within a context of sloppiness on an institutional level. When authority figures within the airline fail to set an example of ideal behavior, deviations become normalized, leading to a degradation in adherence to procedures without individual pilots necessarily being aware of it. Evidence of such high-level normalization of deviance could clearly be seen when investigators monitored TransAsia’s recurrent simulator training sessions. The sessions were dangerously rushed; instructors had only two hours to cover 19 technical subjects and five major maneuvers. And as they hurried through each scenario, the trainees made plenty of mistakes — but so did the instructors. Investigators watched instructors carry out unusual attitude recovery and ground evacuation scenarios incorrectly, and the ASC counted a further 21 procedural errors by trainees which were not corrected by their instructors, ranging from the absence of minor callouts to a loss of altitude during a go-around, a serious event which at most airlines would trigger an internal investigation if it occurred during a real flight. And when all was said and done, the grades given to the trainees seemed completely arbitrary: for example, of two trainees who were observed to be too high during final approach, one failed the check, while the other passed despite ultimately landing too far down the runway, another event which would normally prompt an internal investigation. That instructors would allow such errors to take place without any comment was suggestive of a highly informal working culture that did not take standard procedures seriously.
Meanwhile, investigators began to explore the pilots’ probable mental states at the time of the accident. The cockpit voice recording captured Captain Lee repeatedly yawning, coughing, and sneezing, suggesting that he may have been feeling unwell and was probably suffering from fatigue. At one point he even mentioned that he was tired. Fatigue could explain many of the errors he made during the flight, from his failure to adequately control the aircraft to his repeated selection of improper autopilot modes, which First Officer Chiang repeatedly corrected.
Although it was not possible to determine how much rest Lee got before the flight, his work history showed that TransAsia Airways had been pushing him to the limit for some time.
The problem went back to approximately 2011, when the airline’s leadership began pursuing a strategy of aggressive growth. TransAsia began to push its planes and pilots harder in an effort to complete more flights, carry more passengers, and bring in more revenue. In 2013 and 2014, TransAsia recorded a 9.7% and 15.3% increase in business respectively, but the number of pilots at the airline actually went down by 3.7% during the same period. In the ATR division, pilots were feeling the heat. In 2013, the airline intended to phase out three older ATR-72–500 models in favor of the newer ATR-72–600, keeping a fleet of nine ATR-72s. But the CEO intervened to keep one of the -500 models in service without cancelling the order for its replacement, raising the number of ATRs from nine to ten in order to increase the number of flights that could be conducted. TransAsia needed approximately six pilots per aircraft, but now that they had ten planes in the ATR fleet, they still had only 52 pilots, a shortage of eight personnel.
TransAsia Airways had a hard time hiring new pilots because it did not pay competitively. But instead of increasing wages for pilots in order to attract more talent, management simply forced existing crews to work longer hours. In May 2014, the airline increased the number of flight sectors a pilot could fly in one day from six, the industry standard, to eight, a number which many pilots felt was unreasonable. One TransAsia pilot told the ASC that six sectors was manageable, seven would leave them feeling tired, and eight was practically torture.
Management was aware that pilots were being overworked, but they too were under pressure from company leadership. The head of the Flight Management Department told the ASC that in his line of work, pilots accumulating more than 85 flight hours a month for three or more consecutive months was considered a red flag. In 2014, more than 50% of ATR-72 pilots at TransAsia were working at least that amount, but as long as the schedules did not violate legal duty time limits, his department was simply not allowed to object. The attitude of the executives was that TransAsia Airways should do nothing less than milk its employees to the fullest extent allowed by law.
This relentless pressure inevitably caused pilots to start taking shortcuts and skipping procedures simply to reduce their workload and prevent burnout. One of these tactics was to descend below the MDA in bad weather, allowing crews to get to their destinations more quickly and avoid annoying delays and diversions. TransAsia pilots told the ASC that Captain Lee had done this before, but he was far from the only one. Many experienced pilots violated MDAs on a regular basis, considering it necessary in order to meet the company’s increasingly demanding flight schedules.
In the case of flight 222, Captain Lee had worked several consecutive six- or seven-sector days before the accident, and in the past three months he had accumulated 278 flight hours, close to twice the industry average. He was sixty years old; he seemed to be suffering from a cold or other mild illness; it was dark outside, the weather was bad, and he still had three more flights to complete before he could rest. He was having trouble staying awake and he had been stuck in a holding pattern for the last thirty minutes. It was a perfect storm of conditions, one which caused him to prioritize landing at any cost. Factor in a company culture which had failed to emphasize adherence to procedures, and disaster became almost inevitable.
There were, however, a few additional factors. One of these was the inadequate provision of weather information to the flight crew by air traffic control. Automated equipment had detected a runway visibility range (RVR) well below the minimum in the minutes before the accident, but this information was not given to the pilots. Had they known that visibility was so low, they might have been prepared to abandon the approach much earlier, and Captain Lee might not have thought it was worth it to descend below the MDA if he had known that there was no chance of seeing the runway. The ASC ultimately determined that despite controllers’ belief that the automated sensors were unreliable, the readings they produced on the day of the accident very closely correlated with meteorological conditions observed on airport cameras. The controllers most likely chose to believe a human weather observer over an automated system because of inadequate knowledge of how the system worked.
Investigators also noted that the flight crew did not receive any sort of terrain alarm before the plane collided with trees. As it turned out, the plane simply never entered the envelope in which a warning would have been generated. The Enhanced Ground Proximity Warning System (EGPWS) installed on the plane lacked the precision necessary to define an appropriate warning envelope so close to the airport without generating false alarms during normal approaches. The other possible warnings, “SINK RATE” and “GLIDESLOPE,” could not be generated because the plane never descended at a dangerous rate, and because there was no glide slope, respectively.
EGPWS manufacturer Honeywell noted that a more up-to-date version of its warning system could have provided the crew with a “TERRAIN AHEAD” warning before impact, thanks to a more precise database which allows for a better warning envelope close to the airport. However, this upgrade would have involved hardware changes requiring special approval from the Civil Aviation Authority (CAA), a complex and potentially costly step which TransAsia Airways never considered taking.
By this point it was clear that for the past several years, TransAsia Airways had been an accident waiting to happen. The next question facing investigators was why nobody raised the alarm until 48 people were dead. If the ASC could see these serious problems simply by observing airline operations, then why had the CAA, whose job was to enforce safety regulations, been unable to do the same?
But, as the ASC would soon discover, the CAA’s oversight of TransAsia Airways was both limited in scope and ineffective in practice. CAA inspectors reported that they had a hard time objectively assessing the airline’s cockpit culture because pilots tended to change their behavior when inspectors were present. But the ASC also discovered that CAA inspectors had in fact found repeated violations at the airline, only to give the company the equivalent of a strongly worded letter. On multiple occasions, the CAA informed TransAsia of some sort of problem, the airline replied that the problem would be solved, and the CAA accepted the reply without verifying that anything had actually changed. In fact, the ASC was able to find records dating back years showing that some of the same deficiencies it found during the investigation had been identified by the CAA and “corrected” by the airline, only to continue in practice.
Various internal mechanisms designed to keep the airline accountable to its own safety obligations also proved ineffective. At TransAsia Airways, monitoring of operational safety fell to two departments: the Safety and Security Office (SSO), and the department of Flight Operations Quality Assurance (FOQA). The SSO, however, was tasked with far more than its small work force could handle, including implementing a safety management system, creating the agendas for safety meetings, analyzing quality assurance efforts, conducting operational audits, compiling risk assessments, and more. With the number of employees under its purview, carrying out all these activities properly was impossible.
One of the SSO’s tasks was to conduct self-audits to ensure that pilots were following the rules. But the office’s audit staff received just two hours of training, compared to the industry standard of five days, and were sent off to monitor flight operations with nothing more than a simple checklist. Lacking any relevant expertise and guidance, the auditors proved completely ineffective, routinely failing to notice obvious deviations from standard procedures. Even though deviations were occurring on almost every flight, out of 163 audits between January 2013 and July 2014, only three detected any deviations, and none of these resulted in any corrective actions.
The SSO could have better understood the number of violations through close coordination with the FOQA department, which was supposed to collect flight data and search for exceedances, such as crews who flew too low, landed long, or violated speed limits. However, in practice there was no communication between the FOQA department and the SSO at all. Like the SSO, the FOQA department was grossly understaffed, and there was no one whose job was to coordinate with the SSO. Furthermore, its analysis of data was ineffective because it did not employ anyone outside of management who could speak to pilots involved in exceedances; instead, the interview process was handled by the chief pilot, whose position as the other pilots’ direct boss meant he could never get interviewees to tell the unvarnished truth. The collective result of its inadequate staff and poor organizational structure was that the FOQA department failed to catch on to numerous unsafe trends within the airline’s piloting culture.
Similarly, the Flight Operations department failed to properly assess the risk of an accident due to organizational incompetence. The department had completed a risk assessment based on a list of 13 potential risk factors, but the data used in their calculations was so bad that the findings proved totally useless. The risk factor “non-compliance with standard operating procedures” was based on “self-reports” written up by pilots following the SSO’s “self-audits,” but only 24 of these reports had ever been submitted because most of the auditors didn’t know they were supposed to make pilots file them. And another risk factor, “insufficient manpower,” was set to zero because the assessment was made prior to the airline’s rapid expansion and hadn’t been updated since 2011. The result was that airline management could not quantify the risk they were taking by tolerating a deadly mixture of overwork and disregard for procedures.
All of these organizational deficiencies could have been corrected by consolidating safety-related responsibilities within a comprehensive Safety Management System, or SMS, a structured program designed to systematically analyze operational data, detect unsafe trends, and correct them before accidents occur. A well-run SMS can massively improve safety at an airline. In light of this fact, Taiwan’s CAA had required all airlines to have an SMS by the end of 2012. But while TransAsia Airways had an SMS on paper, it never drafted an implementation plan, nor was it technically required to do so. In practice, the “safety management system” was a vague directive given to the Safety and Security Office which spawned little more than the completely ineffective “self-audits.” Following an inspection of TransAsia’s SMS, the CAA had pointed out several glaring deficiencies, but as it had done many times before, it never checked back to see whether the airline had fixed them. Needless to say, it had not.
When the ASC published these findings in its final report, the CAA immediately went on the defensive, writing that the investigators had fundamentally misunderstood the nature of the SMS regulation, which only required that airlines have a program and did not require the CAA to ensure that the program met any particular standard. The agency’s notification of the SMS deficiencies was therefore purely charitable and they were under no obligation to follow up. Continuing its short-sighted reply, the CAA rejected several ASC recommendations intended to improve the effectiveness of its oversight, and accused the pilots of singlehandedly causing the crash. Because the captain descended below the MDA on purpose, they argued, nothing else about the airline or its oversight mattered. Unfortunately, the CAA’s stance willfully ignored how a company culture can lead pilots to take unacceptable risks.
One would like to say at this point that the CAA’s reply aged poorly in light of later events. But in fact, by the time the reply was submitted, a second tragedy had already proved the ASC right about TransAsia Airways.
On the 4th of February 2015, another ATR-72 operating TransAsia Airways flight 235 crashed into an elevated highway and plunged into the Keelung river shortly after takeoff from Taipei, killing 43 of the 60 people on board. The investigation would discover that the captain shut down the wrong engine after an engine failed during climb. Poor training and inadequate adherence to standard procedures would again be cited as major contributing factors. This second accident forced the CAA to get tough with TransAsia Airways, but it didn’t stop the agency from penning its dangerously short-sighted rejection of the ASC’s findings on the crash of flight 222.
Having suffered two crashes in less than a year, TransAsia Airways quickly entered a financial tailspin. The airline had lost two aircraft, paid out millions in compensation, and undergone several punitive actions by the CAA. The costs, combined with increasing competition, ultimately proved too much to bear. In November 2016 the airline unexpectedly announced that it would cease operations, but not before unidentified individuals sold large amounts of stock in the company, triggering an insider trading investigation. The airline was ultimately dissolved by its shareholders, with the CAA symbolically revoking its certificate of operations the following year.
In the end, the demise of TransAsia Airways provides a stark lesson for airline executives who lack a commitment to safety. In a developed country like Taiwan in the 21st century, even one accident can cripple an airline, and two is all but unthinkable. TransAsia Airways was ruined in the blind pursuit of profit — as were the lives of 91 families, whose loved ones will never return. In this day and age, we know how to run a safe airline, and to ignore that body of knowledge is shameful and reprehensible.
The crash of flight 222 also demonstrates how organizational factors can lead to crashes which are, on the surface, the result of pilot error. By diving into how TransAsia acquired a culture of recklessness and disrespect for standard procedures, the ASC revealed that there were many other hands on the control column as Captain Lee descended below the MDA. And they remind us that standard procedures exist for a reason. As burdensome as it may sometimes feel to brief a familiar approach or make standard callouts, these checks and balances serve to keep pilots in context, aware not only of what the plane is doing, but what risks they will face and how best to mitigate them. If only the crew of flight 222 had thought for a moment about the risk they were about to take, maybe 48 people would still be alive.
_____________________________________________________________
Join the discussion of this article on Reddit!
Visit r/admiralcloudberg to read and discuss over 200 similar articles.
You can also support me on Patreon.
