The near crash of Air Canada flight 759
On the 7th of July 2017, Air Canada flight 759 lined up to land on the taxiway instead of the runway at San Francisco International Airport, in the process coming just seconds away from causing what might have been one of the worst aviation disasters in history. This article examines the sequence of events that brought flight 759 onto a collision course with four other airplanes, and demonstrates just how close it came to catastrophe. In the process it seeks to answer the question of what could have happened, why it did not, and how this near miss has served as an opportunity to prevent future disasters before they occur.

Air Canada flight 759 was a regularly scheduled flight from Toronto, Canada to San Francisco, California, operated by an Airbus A320–200. On board were 135 passengers 5 crew, including a captain and first officer whose names have not been released. The Captain was 56 years old and had more than 20,000 flight hours, including 4,800 on the A320. The first officer, 42, had more than 10,000 flight hours and 2,400 on the A320. They were an experienced team, and the captain had flown to San Francisco many times. Neither had any major training issues, but the first officer had failed an upgrade to captain because he occasionally lost situational awareness and didn’t perform to Transport Canada’s standards.
The night before the flight to San Francisco, the captain slept at home in Toronto. After arriving in Toronto from New York at 23:13, he made his way home and went to sleep between 02:00 and 03:00, then woke up again for the next day’s duty at 07:45, receiving somewhere between 4 and 6 hours of sleep. He didn’t have any flights scheduled that day, but he was on standby in case a backup pilot was needed, and at 11:49, Air Canada called him up to command flight 759 to San Francisco. By the time he reported for duty at 19:40, he had already been awake for nearly 12 hours.
The first officer had gone to sleep at 03:00 the previous night after a flight from San Francisco to Toronto, and woke up at 9:00, getting around 6 hours of sleep. This was similar to the night before that, when he went to bed at 04:00 and woke up at 10:00; in both cases, he was going to sleep very late at night. However, he always napped for 60–90 minutes in the afternoon, while the captain did not.
The times at which the crew last slept are relevant due to the effect of circadian rhythms. A person’s circadian rhythm is their body’s expected cycle of wakefulness and sleep over the course of a 24-hour period. During the day people experience a circadian high that encourages wakefulness, and during the night, from approximately 02:00 to 05:00, people experience their circadian low, the time when the body expects to be asleep. Staying awake during the circadian low causes an elevated level of fatigue, along with all the symptoms associated with it, including forgetfulness, lowered perceptiveness, and lack of focus.

The schedules of both pilots of flight 759 are significant because they were each awake during their circadian low the night before the flight, and the flight to San Francisco would push them into it again. Circadian lows will shift when adapting to a new schedule, but they can’t shift very fast, which results in jet lag when abruptly traveling from one time zone to another. Flight 759 was scheduled to arrive in San Francisco at 23:03 Pacific Time, which was 02:03 Eastern Time (the schedule around which the pilots’ circadian rhythms were based). Therefore, near the end of the flight they would cut into their circadian low and could expect to experience fatigue.
As it turned out, Air Canada flight 759 would not be leaving Toronto on schedule. The aircraft was delayed arriving in Toronto due to weather, so flight 759 wasn’t able to leave until 21:58, more than 30 minutes late. With 140 people on board, the Airbus A320 climbed out of Toronto and began its long cross-country journey toward San Francisco.
Around half way through the five hour flight, as they navigated around mounting thunderstorms, both pilots began to feel fatigued as they approached their circadian low. Unfortunately there was nothing they could do but finish the flight. The plane finally neared San Francisco sometime after 23:30 Pacific Time (02:30 in the pilots’ home time zone).
At the beginning of the flight, the crew received a “notice to airmen” (NOTAM) information sheet which included information about general airport and en route conditions. Included in this NOTAM was an important update: from 23:00 to 08:00 that night and into the next morning, runway 28L at San Francisco International Airport (SFO) would be closed for construction. Crews were working every night for several weeks to resurface the runway and install new lighting, a task which had to be done at night when traffic was low.
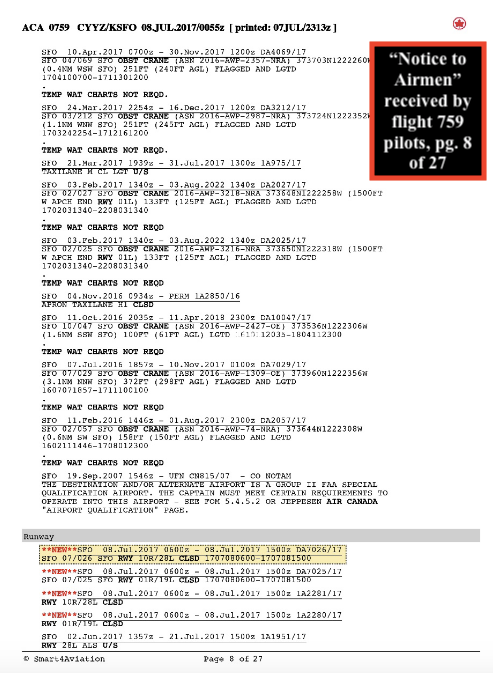
The first officer couldn’t recall seeing the runway closure in the NOTAM. The captain did see it, but at that time he didn’t yet know of the delay and expected to arrive before the closure (even though the scheduled arrival time was 23:03 and the closure was to begin at 23:00). Later in the flight, the captain and first officer briefly discussed the closure, so by the time they began their approach into SFO, they both should have been aware of it. A message was sent to the plane during the flight also containing information about the closure; neither pilot could recall seeing it.
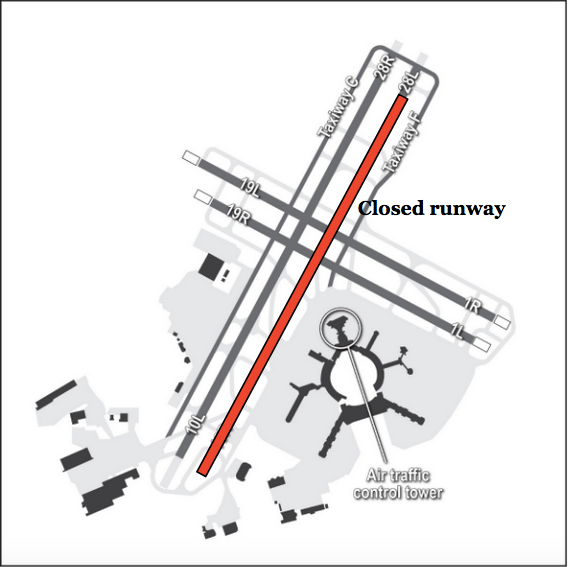
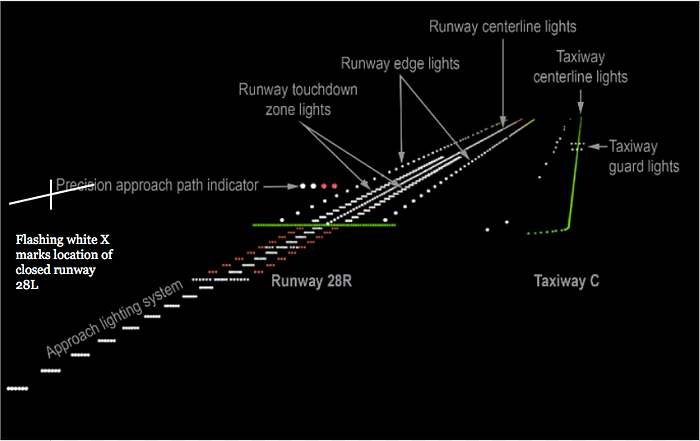
The closed runway 28L had its lights turned off except for a large flashing white X at the runway threshold, and the lights of construction vehicles. This was in accordance with applicable regulations. Runway 28R, running parallel runway 28L, was still in use. And to the right of runway 28R was taxiway C, the route used by aircraft to taxi to the top of runway 28R before takeoff. The lights on 28R were much brighter than those on the taxiway, which was also considerably narrower than the runway.
The air traffic controller at SFO instructed flight 759 to perform an approach called “Quiet Bridge,” which overflew several major bridges in San Francisco Bay before lining up with runway 28R. Although this was a visual approach, flown manually using landmarks, the procedure outlined in the approach chart called for pilots to tune their navigational equipment to the frequency of the instrument landing system (ILS) for runway 28R to help them line up with the runway, even though the ILS would not actually be used. However, the first officer never entered the frequency, and neither pilot checked that the frequency appeared on their displays, even though they were supposed to. The first officer was unable to explain how this could have happened, but it seems likely that the pilots were suffering from fatigue and were not fully processing the charts they were reading. This was exacerbated by the fact that the Quiet Bridge approach was the only approach flown by Air Canada that required manual tuning of the ILS frequency.
In line with Air Canada policy, the pilots then discussed potential threats to the approach. They touched on topics including nearby mountains, nighttime visibility, other traffic, and their own fatigue. However, neither of them mentioned the fact that the adjacent runway 28L was closed and would be mostly unlit. Apparently they had forgotten.
Ahead of them, Delta Airlines flight 521 was coming in to land on the same runway using the same approach. Its pilots faced a confusing sight: they thought they had lined up with runway 28R, but they appeared to be lined up with runway 28L instead. The source of the confusion was simple: with runway 28L unlit except for the white X, runway 28R and taxiway C looked like runway 28L and runway 28R respectively. Pilots flying into SFO were used to seeing two parallel runways, and under these circumstances the parallel runway and taxiway gave off the illusion of being the expected parallel runways. The crew of flight 521 checked their navigation equipment, confirmed they were lined up with the correct runway, and proceeded to land without incident.
Meanwhile, the pilots of Air Canada flight 759 were about to be hit with the same illusion — but without the benefit of their navigational aids. And the captain had been awake for 19 straight hours.
Less than 15 minutes before midnight, one of the two air traffic controllers working the SFO control tower left the building to take an official “recuperative break.” This left just one controller handling all air and ground traffic in and around the airport. This was only allowed when traffic was light. If planes had to wait in line to take off, then traffic was considered too heavy for a single controller to be on duty. Although the controllers assessed traffic to be light when the second controller went on break, in fact at that moment there were four planes making their way up taxiway C to await takeoff from runway 28R after Air Canada flight 759 had landed on it.
At 23:46, the lone controller cleared flight 759 to land on runway 28R. Now on final approach, the captain of flight 759 made a short left turn to line up with the runway. Suddenly faced with the illusion of two parallel runways, he instinctively lined up for the “runway” on the right, which was actually taxiway C!

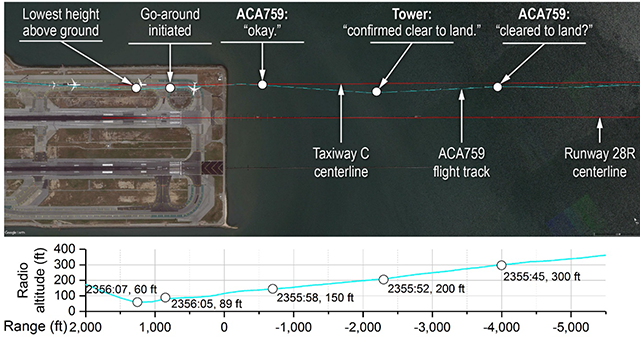
At the moment that the captain lined up with the taxiway, the first officer had his head down programming in the heading and altitude for a missed approach, so that it could be quickly selected if they had to go around and try again. Immediately after this, he had difficulty finding the runway heading in his charts. Therefore he wasn’t looking at the runway when the captain lined up with it. However, as flight 759 descended through 600 feet, the captain thought he saw something unusual on the “runway” ahead of him. He asked the first officer to contact the controller and make sure there wasn’t a conflict.
The first officer said to the controller, “Uh, Tower, I just want to confirm — this is Air Canada 759 — we see some lights on the runway there, across the runway. Can you confirm we’re cleared to land?”
The controller scanned his ground radar, which showed the locations of vehicles and airplanes within the airport, and saw no conflicting traffic on the runway. “There’s no one on two eight right but you,” he said to flight 759, which was then descending through 200 feet. He saw that the plane was aligned slightly to the right of the runway, but this was not unusual, and at such an oblique angle he could not tell that the plane was in fact aligned with the taxiway.
In the cockpit of flight 759, both pilots began to feel a growing apprehension that something was wrong. They couldn’t see any planes in their path because their wing and tail lights blended in with the edge and centerline lights of the taxiway, and yet there was definitely a sense that something was very much not right.
Some of the crews waiting on the taxiway had already realized exactly what was happening. At the head of the line was a United Airlines Boeing 787 Dreamliner, operating United Airlines flight 1 to Singapore. The captain of flight 1 had a clear view of flight 759, and at first he, like the controller, saw that it was headed toward the taxiway but initially assumed that it would realign itself. But as the A320 drew nearer and nearer without changing course, he finally keyed his mic on the tower frequency and said, “Where’s this guy going? He’s on the taxiway!” At the same time, the crew of Philippine Airlines flight 115, an Airbus A340 bound for Manila, turned on its bright landing lights to try to alert flight 759 to the danger.
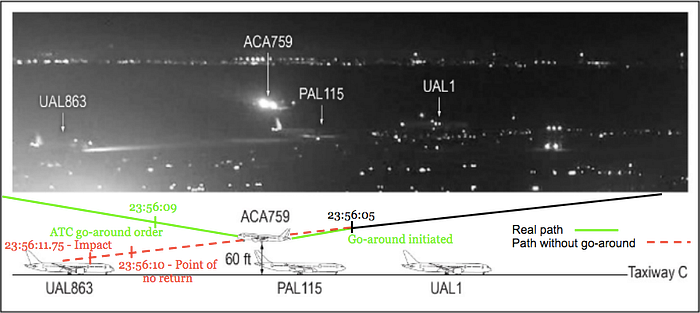
The controller didn’t know who made the transmission and it seemed out of context. He momentarily muttered to himself, “Who is talking?” At that point he noticed that the position of Air Canada flight 759 looked “very strange.” Flight 759 overflew United Airlines flight 1 at an altitude of 100 feet and kept descending, headed straight for the Philippine Airlines A340. But with its landing lights on, the huge A340 was almost impossible to miss from such a close vantage point. At an altitude of 84 feet, both pilots on flight 759 called for a go-around simultaneously, and the captain advanced the throttles to abandon the approach. While the engines spooled up, the A320 dropped to a low point of about 65 feet, coming a hair’s breadth from clipping the 55-foot-tall vertical stabilizer of Philippine Airlines flight 115. Four seconds after flight 759 starting going around, the controller also ordered a missed approach, though by this time the A320 was already climbing. Passing back up through 200 feet, flight 759 then overflew another United 787 bound for Sydney and a United 737 bound for Cancún.

As flight 759 flew away from SFO to line up again, United flight 1 radioed the controller and said, “Air Canada flew directly over us.”
“Yeah, I saw that, guys,” said the controller. To flight 759, he said, “It looks like you guys were lined up for Charlie.” No one yet knew just how close they had come to disaster.
A few minutes later, Air Canada flight 759 landed normally on runway 28R and taxied to the gate. The passengers walked off and went home or to their hotels with no knowledge of the events that had transpired. The pilots discussed the flight, telling another pilot that they had almost landed on the wrong runway, then filed an Air Canada incident report which correctly stated that they lined up with the taxiway. The crew flew the return flight to Toronto the next day before Air Canada got wind of the incident and took them off flying duty, pending an investigation.
The National Transportation Safety Board didn’t find out about the incident until several days later, by which time the cockpit voice recording from flight 759 had long since been erased. However, flight data was still available, and it showed a picture of a closer call than anyone had imagined. And that meant that new safety measures were needed to prevent a repeat incident that could potentially claim hundreds of lives.
To illustrate how things might have gone differently, I used flight 759’s published ground speed and descent rate figures to calculate what might have happened if the pilots began the go-around just a few seconds later. In the 13 seconds before the go-around was initiated, the A320 was descending at a rate of about 8.5 feet per second with a ground speed of about 200 feet per second. This would have been just enough to miss the 55-foot-tall tailfin of the Philippine A340, assuming the pilots didn’t change their groundspeed or descent rate. Less than seven seconds after the time of the actual go-around, flight 759 would have slammed headlong into the roof of the Sydney-bound United Airlines Boeing 787. Since the plane kept descending for two seconds after beginning the go-around, it can be concluded that if the crew had delayed their go-around by just five seconds, they would have collided with the 787. The controller ordered the go-around four seconds after the pilots initiated it. Therefore, if the pilots had relied on the controller’s order, they would have had only one second to avert disaster. There is reason to doubt that this would have been sufficient.
If flight 759 had collided with the roof of the United 787, it would have easily ripped through the top of the cabin, crushing many of its occupants and leaving the survivors with only a narrow window to escape the inevitable inferno. The rear of the plane would likely have been totally destroyed. The main body of the Air Canada A320 would then have continued onward, striking the United 737 head-on only one or two seconds later. Both aircraft would likely have been destroyed by the impact or by fire with few, if any, survivors. The number of people on board the 787 and the 737 is not known, but if both were at 75% capacity, then the death toll could have been as high as 460. If both planes were full, then it could have rivaled the Tenerife Disaster.
The deciding factor that kept this catastrophe in the realm of alt-history, and not real history, might have been the actions of the pilots lined up on the taxiway. Because the captain of United Airlines flight 1 was watching flight 759 come in to land, he realized that it was aligned with the taxiway and transmitted a warning on the tower frequency, which was heard by the Air Canada pilots. At about the same time, the pilots of Philippine Airlines flight 115 turned on their bright landing lights, making their aircraft more easily visible. The combination of these two acts were sufficient for the Air Canada pilots to realize something was wrong and initiate the go-around. Notably, the pilots sounded shocked when told later that they had overflown aircraft on the taxiway, suggesting that they never actually saw any of the four planes. In fact, it was a general sense that something was wrong that prompted them to go around, rather than a sighting of an imminent collision. If the United captain had not said “Where’s this guy going? He’s on the taxiway,” then they might not have realized the need for a go-around until the controller commanded it, by which point it could have been too late.
The question had to be raised: how was it possible to line up with the taxiway instead of the runway? In fact, in the previous 12 years there had been two cases of airliners actually landing on taxiways at major US airports. In both cases there were no obstacles, and the planes rolled out safely and taxied to their gates before anyone realized what had happened.
This is despite that fact that, in theory, a taxiway and a runway don’t look very similar. The runways at SFO have high-power approach lighting mounted on a pier extending out from the runway threshold; the taxiway does not. The taxiway is less than half as wide as the runway. Its centerline is green instead of white. All its lights are noticeably dimmer. The runway has touchdown zone lights, but the taxiway doesn’t. And yet, the crew of Air Canada flight 759 was not the only crew landing at SFO that night who encountered confusion about which one was runway 28R! The answer lies in two phenomena: fatigue, and expectation bias.
The first is relatively simple. Neither pilot got a full 8 hours of sleep the previous night, and both reported feeling tired well before the approach into San Francisco. Having been awake for 19 hours, there was no way the captain’s perception, awareness, and reaction times were not beginning to degrade. The first officer was more rested but also reported feeling tired, which likely contributed to his failure to notice the unusual requirement to manually tune the ILS for the Quiet Bridge approach. Had they tuned the ILS, the experience of Air Canada flight 759 would have been no different from the Delta flight that landed ahead of it.
The fatigue also worsened the effect of the second major psychological factor, expectation bias. The pilots had not assimilated the information regarding the closure of runway 28L, which was buried in the middle of the NOTAM amid a large amount of less important information. This information was similarly indistinguishable in the automatic message they received later in the flight. Although at one point they apparently knew of the closure, they appear to have forgotten by the time they began their approach, because neither pilot mentioned it during the briefing or the discussion of threats. Therefore they were not mentally prepared to see only one runway, and subconsciously expected to see the two parallel runways they had encountered every other time they flew to SFO. This expectation bias was so powerful that it overrode numerous conflicting signs, including the different lighting of the runway and the taxiway, as well as the large illuminated X at the threshold of runway 28L. Contributing to this were a small number of supporting clues, including the wingtip lights of the airplanes appearing to widen the taxiway, and the lights of the construction equipment on 28L appearing similar to airport infrastructure. Furthermore, the first officer only looked up after the captain had aligned with the taxiway, and the expectation that the captain would align with the runway inhibited his ability to assimilate information that suggested otherwise.

The NTSB also found numerous points at which the incident could have been averted before anyone was in danger. The Enhanced Ground Proximity Warning System (EGPWS) on board the Air Canada A320 offered an optional feature called SmartLanding, which would have sounded a warning that the plane was attempting to land on the taxiway. However, this feature was not installed. Secondly, ground radar installed at the airport could only warn the controller of potential collisions between aircraft and vehicles on the ground, and could not predict a collision involving an aircraft coming in to land. During the investigation, the NTSB showed that the system could be effectively reprogrammed to warn of such collisions. Third, given the number of planes waiting to take off, there should have been two controllers in the tower; having only one controller handling ground and air traffic cluttered the radio frequency and delayed flight 759’s inquiry about the runway conditions.
Furthermore, Air Canada had recently rolled out a training lesson focused on how to recognize and overcome expectation bias, including how to listen to “gut feelings.” However, the pilots of flight 759 had not yet received this training. And most importantly, the rest that the pilots received in the days before the incident, while insufficient, was not out of line with Canadian duty-time regulations. Despite research which shows that fatigue-induced errors begin to increase after a pilot has been awake for 11 hours, Canadian pilots were allowed to be on duty for up to 14 straight hours, plus an additional 3 if “unforeseen circumstances” arise. It would therefore have been legal to keep the flight crew on duty for up to 9 more hours after they arrived in San Francisco! In fact, the NTSB showed that these pilots’ schedule would not have been allowed in the United States. In the US, reserve pilots must be notified at least 12 hours before they are asked to operate a flight that continues into their natural circadian low; Canada had no such rule, and the captain had less than 8 hours’ notice. Furthermore, in the US, time on duty was measured from the moment the reserve pilot became available for duty, not when they actually were called up. Under this rule, the captain would not have been able to complete flight 759 within duty limits. At the time, Transport Canada was considering stricter pilot fatigue standards, and the NTSB recommended that they implement them as soon as possible.

In its final report, the NTSB made numerous recommendations intended to prevent the next incident like Air Canada flight 759 from ending in disaster. The Safety Board asked that airlines find ways to eliminate or better highlight approaches that require unusual manual frequency inputs; that experts review ways to better present information to pilots in NOTAM, ATIS, and ACARS messages; that aircraft have a system that warns when the plane is aligned with a taxiway; that airport collision detectors be able to detect collisions involving landing aircraft; that closed runways be made more conspicuous; and that Transport Canada revise fatigue rules for Canadian pilots. The NTSB also expressed concern about the amount of time taken for the pilots to report the incident and for the NTSB to be notified, resulting in the erasure of the cockpit voice recording.
In their closing statements, members of the investigation team reflected on the opportunity to recommend major changes before an accident actually occurred. “This incident report should be required reading for all pilots,” wrote Vice Chairman Bruce Landsberg. “Only a few feet of separation prevented this from possibly becoming the worst aviation accident in history.”
“I am not comforted because … everyone made it home safely,” another investigator wrote. “I believe more robust measures should be in place to intervene when a dangerous situation becomes apparent.”
Closing out his statement, Landsberg added, “Everyone will gain much more from being introspective rather than judgmental on this incident. We should reward all aviation personnel and celebrate when someone self-confesses a mistake and learns from it. It’s almost a certainty this crew will never make such a mistake again and my hope is that they will continue to fly to the normal end of their careers.”
_______________________________
Visit r/admiralcloudberg on reddit to view all 100+ articles in the plane crash series. Thank you for reading.
