Acids to Ashes: The crash of Pan Am flight 160

On the 3rd of November 1973, the crew of a Pan Am cargo plane lined up to land at Boston’s Logan International Airport, struggling desperately to reach the runway as a fire raged in the cargo deck and smoke filled the cabin. But just moments from touchdown, the aircraft appeared to sway wildly from side to side before it abruptly dived into the runway threshold, spewing burning debris across Logan’s runway 33 Left. None of the three crew survived to explain why.
The investigation into the crash revealed a sequence of events that touched multiple areas of the aviation industry, from supply line confusion involving a massive shipment of corrosive chemicals, to the design assumptions built into the Boeing 707’s firefighting procedures, to crew resource management issues, as the flight engineer turned off critical control systems without the captain’s knowledge. Piecing the details together wasn’t easy, even with the help of the sometimes vague NTSB report. But while some questions remain incompletely answered, the story of Pan Am flight 160 nevertheless highlights the fallacy underlying several safety assumptions that were not properly questioned until the crash of UPS flight 6 in 2010. In fact, those very parallels are part of what make this obscure 50-year-old accident worth revisiting — because some of the mistakes that brought down flight 160 transcend the time period in which they occurred.
◊◊◊

Between 1956 and 1983, Pan American World Airways, the de facto flag carrier of the United States at the time, operated a cargo division specializing in international freight transport to and from the US. During the 1960s and 1970s, the workhorse of the Pan Am Cargo fleet was the -320C variant of Boeing’s first jet airliner, the four-engine 707. The 707–320C had a strengthened floor and a new cargo door to permit cargo-only operations, with a cabin that was fully convertible between passenger and cargo configurations, as well as intermediate or “combi” formats. However, the 707 that starred in this particular story was configured for cargo only.
That aircraft, with registration N458PA, was manufactured in 1967 and had been in service for 6 years when it arrived at the cargo loading ramp at New York’s John F. Kennedy International Airport on the 3rd of November, 1973. Its next scheduled trip was flight 160 to Frankfurt, Germany, with a stop at Glasgow Prestwick Airport in Scotland, where personnel were to offload several pallets of material bound for the National Semiconductor manufacturing plant in nearby Greenock.
Now a division of Texas Instruments, the National Semiconductor Corporation, or NSC, was a major independent manufacturer of semiconductors and related analog devices, headquartered in Santa Clara, California.
The semiconductor manufacturing process involves a laundry list of caustic chemicals with scary names that I won’t enumerate, but it’s a fact of our modern world that sometimes these chemicals have to be transported from one place to another. And it was also a fact that sometimes NSC needed to buy chemicals in America for later use at its Scottish facility. It would be possible to ship them by water, but in a high-tech industry like semiconductors, putting the materials on a cargo ship is sometimes too slow, so only an airplane will get the job done in time. And for this particular mission, who else but Pan Am?
In September and October 1973, NSC placed several orders for various chemicals from the Allied Chemical Corporation, or ACC, which is now part of Honeywell.* ACC acted as a one-stop-shop to buy chemicals that were mostly manufactured by other companies. The chemicals in NSC’s orders that were bound for the Scotland plant via Pan Am flight 160 included but were not limited to butyl acetate, stripping solution A-20, isopropanol, hydrogen peroxide, xylene, acetone, nitric acid, methanol, hydrofluoric acid, sulfuric acid, and glacial acetic acid. In its order request, NSC specified that the chemicals needed to be properly packaged for air transport, an area where ACC needed outside assistance. Given the large number of chemicals in its inventory, the company didn’t necessarily have the expertise on hand to safely repackage every chemical for every mode of transport.
An ACC manager subsequently attempted to engage another chemical company to repack some of the chemicals that were stored in containers that exceeded the maximum quantity restrictions for air transport. However, the other company, which was not named in the report, replied that they were “not interested.” My understanding is that repacking these chemicals into smaller containers is a rather complex and potentially dangerous process, and this third company probably decided that the liability wasn’t worth it.
On October 25, ACC advised NSC that while they were aware that the chemicals would be shipped by air, they would nevertheless be packaged for surface transport. Now, this is where matters become slightly confusing.
To understand why, we need to talk about nitric acid, which is the chemical of primary interest to this story. Nitric acid (HNO3) is a corrosive mineral acid and an oxidizer that will react with a wide variety of substances, producing heat and oxygen as byproducts. It therefore presents not only a corrosion risk but also a fire risk — in fact, even though the acid itself isn’t flammable, it’s such a powerful oxidizer that some fuels will ignite immediately upon contact with it. For this reason, in 1973 federal regulations required that bottles of nitric acid intended for transportation “be placed in tightly closed metal containers, and well cushioned therein on all sides with incombustible mineral packing material, such as whiting, mineral wool, infusorial earth (kieselguhr), asbestos, sifted ashes, or powdered china clay, etc.”
*Actually, AlliedSignal, the successor of ACC, acquired Honeywell and adopted its name, not the other way around. I have to put this in here because my readers are pedants. I say that with love.
Neither the NTSB report nor the reproduced text of the regulation states what type of transportation the above packaging was required for. I was also unable to find the original version of the federal hazmat regulations that were in force at the time. It appears most likely, from context, that these regulations did apply to transport of nitric acid by air, and the NTSB report states that there were generally few differences between the packaging requirements for chemicals shipped by cargo plane and those shipped by freight rail. However, any differences between packaging requirements for aircraft versus truck transportation are not mentioned in the report. Since ACC intended to ship the nitric acid to Pan Am’s JFK loading facility via truck, it can be presumed that when the company said it would package the nitric acid “for surface transport,” it was following or attempting to follow the packaging regulations for truck transportation. However, I was not able to find these regulations or establish whether they differed from air transport packaging requirements in any way.
One might presume that the main difference was the container size — after all, ACC had tried and failed to find a contractor who could repack some chemicals whose containers exceeded the maximum unit volume for air transport. However, according to the Pan Am flight 160 cargo manifest, the nitric acid was stored in 5-pint bottles, which are smaller than the maximum per-container quantity of 2.5 L prescribed by current US hazmat regulations for air transport. This volume presumably was within limits in 1973 as well, although this is not explicitly discussed in the NTSB report. Therefore, it remains unclear what ACC meant when it said it would package the nitric acid for surface transportation but not for air transportation.
It is also not precisely known, or at least the NTSB report does not make it precisely known, how ACC originally packaged the nitric acid, except that the acid was stored in glass bottles with plastic screw-on caps. It is known that the bottles were not placed in metal containers as required by the hazmat regulations for air transport. I wasn’t able to determine whether such containers were required for truck transport at the time. What materials were used to cushion the bottles at this stage, if any, is also not stated in the report. However, we’ll come back to that topic in a moment.
To deliver the nitric acid and other chemicals from its facility in southern California, ACC contracted the trucking company P. Calahan Inc. to transport the goods to Maspeth, New York, where they were to be deposited at a “repacking and trucking facility” owned by the logistics company Seven Santini Brothers. NSC had verbally contracted Santini to repackage the chemicals before transferring them to the Pan Am cargo loading facility at JFK Airport. It isn’t explicitly stated why this was done but I presume that NSC’s intention was for Santini to upgrade the packaging to meet air transport requirements after learning that ACC would not do so. At this point Santini should probably have asked NSC for detailed handling instructions, but they didn’t, and even if they had, NSC’s traffic manager possessed no such information anyway.
When the nitric acid and other chemicals arrived at the Santini facility, the Santini office manager consulted the International Air Transport Association (IATA) Restricted Articles Regulations in order to determine what types of packaging and labeling would be needed. He did not appear to be aware that IATA rules, while helpful, carried no legal force in the United States, and that FAA and Department of Transportation regulations had to be consulted as well. Nor did he appear to understand much of anything else about transporting hazmat.
Here is where we have to come back to the question of how the nitric acid bottles were cushioned, and by whom. What we know for sure is that by the time the bottles reached the aircraft, they were cushioned with sawdust, which clearly doesn’t meet the regulatory requirement that nitric acid bottles be packed with an “incombustible” cushioning material. So who put the sawdust there? The NTSB report is somewhat open to interpretation on this matter.
When discussing the packaging worksheet put together by the Santini office manager, the NTSB report states, “it was presumed by the packer that if [sawdust] was ‘OK’ for red label materials, it was ‘OK’ for white label materials.” So what does that mean?
There are several possible meanings of “red label” and “white label,” and the NTSB report doesn’t clarify which. It could be that the labels refer to a labeling system that existed in 1973 but is no longer in use; however I have not identified any such systems.

The possibility I prefer is that “red label” and “white label” refer to two of the four NFPA 704 label colors that are used to quickly convey information about the type of hazard posed by a chemical. Appearing in a diamond shape, the four colors — red, blue, yellow, and white — indicate, respectively, the chemical’s flammability, hazard to health, reactivity, and any other special properties it may possess. The red, blue, and yellow labels are accompanied by a number on a scale from 0–4 indicating the seriousness of the threat. The white label conveys other information using one of a small number of special symbols, including OX for an oxidizer.
It would be somewhat strange for the report to refer to “red label materials” or “white label materials” when discussing NFPA 704, since all four colors always appear on the label and it’s the number or symbol that indicates the level of danger. However, this statement isn’t a direct quotation from any of the individuals involved, and if we assume it got mangled somewhere between the packer’s original understanding and its description in the NTSB report, then an intriguing explanation makes itself apparent.
The issue is that nitric acid will happily react with the organic compounds in sawdust to produce heat and oxygen that then combine to set the sawdust on fire. However, because the acid itself isn’t flammable, its NFPA 704 red label has a value of zero, indicating “not flammable.” Therefore, it’s plausible that the packer knew sawdust was an approved cushioning material for substances with a red label value of zero, and consequently believed that sawdust was an approved cushioning material for nitric acid bottles, even though the white label indicated that nitric acid is an oxidizer. To date, this is the only plausible explanation I’ve come up with for why someone would think sawdust was okay for this purpose.
But even then, we’re still left with another glaring question: who was the “packer” who made this mistake? Unfortunately, the NTSB report isn’t clear about this matter either. One possibility was that “the packer” referred to Santini. But I think the evidence actually suggests that the packer who became confused about labels was ACC itself.

On this matter, a crucial line in the report states, “Since Santini did not stock noncombustible cushioning material and had no metal cans to encase the nitric acid, the Lyon representative was contacted.” The middle part of this line makes it clear, as I stated earlier, that ACC placed the nitric acid bottles directly in the boxes without intermediate metal cans before sending them to Santini. Otherwise there would have been no need for Santini to provide its own metal cans.
However, the first part of this line has multiple interpretations. First of all, if Santini was contacting a third party for advice because they didn’t have noncombustible cushioning materials, it follows that the Santini office manager knew or suspected that noncombustible cushioning material was required to pack the nitric acid. Furthermore, one of three possibilities must be true: 1) the nitric acid as received by Santini was already cushioned in sawdust; 2) the nitric acid was received without cushioning material at all; or 3) the nitric acid was received with noncombustible cushioning material, but Santini was unable to reuse the material. We know that one of these must be the answer because if the nitric acid had arrived with reusable, noncombustible cushioning, then the fact that Santini didn’t have noncombustible cushioning was irrelevant.
Now, before trying to determine which of these possibilities is most likely, we need to explain who Lyon was and what they told Santini. This third party was Lyon Commercial and Export Packing Division, which had been contracted by NSC to pick up and pack 60 boxes of sulfuric acid from ACC in southern California. Lyon had then delivered the boxes to Burlington Northern Air Freight, which packaged them for air transport and handed them to TWA, which flew them to JFK. Lyon wasn’t involved in shipping any of the chemicals that ended up at Santini, but apparently they were being used as a point of contact. And when the Santini office manager telephoned Lyon for advice about the nitric acid, the Lyon representative told him that it was perfectly fine to omit the metal canisters and use sawdust as packing material. This was completely, wildly, pants-on-fire false. However, the office manager did what he was told, and the repackaging worksheet given to the floor personnel consequently instructed them to place the glass bottles of acid directly into the wooden boxes and cushion them with sawdust.
This phone call is quite clearly the reason why Santini believed sawdust was an acceptable cushioning material. However, if we follow possibility 2 (the nitric acid was received without cushioning material) or possibility 3 (the nitric acid was received with noncombustible cushioning material that could not be reused), then Santini is the party that first introduced the sawdust, and therefore must also be the “packer” who thought sawdust was okay because nitric acid has an NFPA 704 flammability score of zero. But that’s not why Santini thought sawdust was okay — they thought that because Lyon told them it was. So Santini can’t be the “packer.” And the “packer” can’t be Lyon because they didn’t pack the nitric acid at any point. So the packer who was confused about labels has to be ACC, and therefore the answer must be possibility 1 (the nitric acid as received by Santini was already cushioned in sawdust).
As for why ACC, a chemical distributor, would make this mistake, it’s easier than you might think. Today, people involved in handling hazmat can refer to the Material Safety Data Sheet for detailed instructions, but the MSDS wasn’t created until 1983. And remember, ACC didn’t manufacture chemicals — they had an inventory of thousands of chemicals manufactured by other people. So one can imagine a poorly trained floor employee misreading the NFPA 704 and packing nitric acid in sawdust because the little diamond said it wasn’t flammable. The bottles cushioned in sawdust were then shipped across the country to Santini, where the office manager saw them, thought “that’s weird, shouldn’t the cushioning be noncombustible,” and then called Lyon, who told him it was fine as-is.
None of the information in the above paragraph is clearly or directly stated in the NTSB report. However, I think it’s the most likely explanation for what happened, based on the available evidence.
◊◊◊

Working from the office manager’s instructions, Santini personnel constructed wooden boxes according to the specified federal standard, placed the nitric acid bottles and sawdust cushioning into the new boxes, and organized the boxes onto pallets for transportation by truck to JFK. Santini did not affix labels stating “corrosive liquid,” “cargo aircraft only,” and “this end up,” even though these were specified in the IATA rules used by the office manager to create the packaging worksheet. In this condition, the nitric acid and other chemicals were taken to the Pan Am loading dock on November 2nd, the day before flight 160’s scheduled departure, where the shipment was united with the sulfuric acid shipment from TWA.
The chemicals purchased by NSC represented only part of the cargo to be carried on flight 160. Out of 24,000 kg of cargo, only about 7,000 kg were restricted chemicals; the rest consisted of various merchandise, machinery, and mail, which collectively occupied 10 out of the aircraft’s 13 available cargo loading positions. Pan American attempted to organize the shipment onto three pallets to fit the remaining three positions, but the loaders discovered that not all of the chemicals would fit on three pallets. This was probably because the sulfuric acid was supposed to have been shipped via TWA on October 31st but was bumped to flight 160 at the last minute after the required space failed to materialize. To correct the issue, the loaders removed some items from a fourth pallet and replaced them with several boxes that may have contained sulfuric acid.
But when Pan Am ramp workers tried to load the three remaining pallets onto the aircraft, they found that the outer edges of the upper tier were not sufficiently contoured to fit into the 707’s cylindrical fuselage. If the stack of boxes on the pallet is too square, the upper corners won’t fit through the opening, which is exactly what happened in this case. So in order to make the topmost tier of each pallet narrower, the supervisors on duty instructed the cargo loading personnel to turn some boxes on the topmost tier sideways. Although the nitric acid boxes did have small arrows pointing upward on each face, recall that Santini hadn’t affixed them with the required “this end up” labels. And considering that there were no less than 160 nitric acid boxes in the NSC shipment, amounting to almost half the total, it was virtually certain that some of the boxes that were upturned by the Pan Am cargo loaders contained nitric acid.
The first shift to work on the pallets bound for flight 160 didn’t quite finish the job, and when the second shift arrived to find boxes on their sides, one employee became concerned and took the issue to a supervisor. However, the supervisor told the employee to leave the boxes that way, and the matter was closed. A short time into this second shift, the pallets were finally wrapped and covered, and a walkaround inspection identified no spillage or unusual smells. The pallets were then loaded onto the 707’s main deck.
According to federal regulations, flight crews must be notified of any restricted cargo aboard their aircraft so that they can use this information for things like emergency decision-making and notifying fire crews. These regulations specified that the dispatcher or person in charge of cargo palletization must sign a notification document listing the amount and type of hazmat on the aircraft, which was to be presented to the captain by the loadmaster. The captain was required to sign the notification, demonstrating their acceptance of the cargo (or, should the captain identify some problem with the hazmat, this would provide a final opportunity to reject the shipment).
In the case of Pan Am flight 160, the hazmat notification was signed by the dispatcher, but was never given to the loadmaster, who was only barely aware that there was hazmat on board at all. Instead, the notification was handed to another unspecified individual, who claimed that he presented it to the captain, then left the documents aboard the aircraft. But while one page from this notification was later found in the wreckage after the accident, the captain’s signature wasn’t on it — and as we will soon see, the actions of the crew during the flight did not suggest that they were aware of the hazmat lurking in the main deck cargo area.
◊◊◊
The crew of Pan Am flight 160 consisted of two pilots and a flight engineer, led by 53-year-old Captain John Zammett, a highly experienced airman with over 16,400 flying hours, including over 5,800 on the Boeing 707. The first officer was 34-year-old Gene Ritter, who had been flying for Pan Am since 1966, accumulating a total of 3,843 flying hours, all of them on the 707. And lastly, the flight engineer was 37-year-old Davis Melvin, who had over 7,200 hours, including 3,260 on the 707. Without going into excessive detail, it suffices to say that this was a crew who knew the 707 inside and out.
At 08:25 local time, flight 160 took off from JFK and headed northeast across New England and Canada. For the first half an hour, there was no sign of trouble. But the apparent quiet belied the dangerous situation developing on the cargo deck.
The NTSB could only guess at what exactly happened, but the theory goes as follows. Most likely, the caps on the nitric acid bottles were screwed shut at sea level, with no pressure differential between the inside and outside of the bottle. But while the 707’s main deck is pressurized, it’s not pressurized to sea level, so as flight 160 climbed, a pressure differential would have developed between the inside and outside of each bottle. This wouldn’t have been a problem in bottles that were stored upright, due to the layer of air between the top of the acid and the bottom of the lid. But if a jar was turned sideways with the acid directly against the lid, and the lid was only “sea level tight,” then the pressure differential could have forced some of the nitric acid out the bottle through tiny gaps under the seal. If you’ve ever driven up a mountain with a reusable water bottle, and it started squealing and foaming, that’s the same phenomenon.
If nitric acid began to leak in this manner, it would have come into direct contact with the sawdust cushioning material due to the lack of intermediate metal canisters. In NTSB tests, sawdust exposed to nitric acid began to produce white smoke after 7 minutes, and flames became visible after 19. Two minutes after that, the flames escaped from the box. At that point, if the box had been aboard a real cargo plane, the fire would have become uncontrollable.
At some point as flight 160 was climbing to its cruising altitude of 31,000 feet, one of the upturned nitric acid bottles most likely leaked into the sawdust, triggering a reaction that generated heat and oxygen until something caught fire.
Although the 707–320C was equipped with main deck smoke detectors, the NTSB found that they didn’t provide early warning of the fire, for unknown reasons. The smoke detectors on the 707 were a primitive design in which air from the compartment was physically drawn past a window in the flight engineer’s station, where smoke particles were illuminated by an indirect light source, creating the impression that the window was lit. A small pinhole above the window allowed the flight engineer to check whether the indicator bulb was working. Unfortunately, this setup was much less reliable than a smoke detector located in the compartment itself, and there are many plausible reasons for its failure to provide a timely warning.
The cockpit voice recording only captured the last 30 minutes of the flight, which didn’t include the pilots’ initial observation of smoke. Rather, the first conversation on the CVR consisted of Captain Zammett calling the Pan Am operations department for advice. “Ah, yes sir, we have ah, accumulation of smoke in the lower 41 and we’re gonna go back to Boston. Do you want us back in Boston or back in New York?”
“Ah, standby 160, we’ll find out,” Operations replied.
The “lower 41” was a term used by 707 pilots to refer to the avionics bay, which was located underneath the forward galley and aft part of the cockpit. The cramped compartment could be reached by a crew access hatch in flight. It was also connected to the cockpit by a floor vent designed to prevent a pressure differential from developing between the two spaces. Cooling air to the avionics was supplied by a cooling fan that also drew air down from the cockpit into the compartment.
If the crew thought the lower 41 was the source of the smoke, then it must have been because it was the first place they saw smoke, probably swirling about near the floor vent. It is known that this smoke came from the fire in the main cabin, but how it got there is somewhat unclear from the NTSB report. According to the 707–320C operations manual, airflow into the underfloor avionics bay comes from the cockpit and is exhausted either directly from the compartment via the electronic cooling air valve, or indirectly via ducts leading around the outside of the forward (lower) cargo compartment and out through the forward outflow valve. I wasn’t able to find any reference to a normal airflow path from the main deck into the lower 41 that could have caused smoke to be drawn there.

The NTSB report states that during post-accident smoke tests, “airflow was observed to move downward through the barrier smoke chute into the lower 41.” The “barrier” appears to refer to a “smoke barrier” installed between the main deck cargo area and the crew rest area behind the cockpit. However, I wasn’t able to find any reference to this barrier or a “smoke chute” anywhere in the operations manual, and the location, nature, and purpose of these components was not explained in the NTSB report.
Furthermore, an annex to the report states, “The Boeing Company has issued [a] Service Bulletin… which permits installation of a smoke chute in the passenger-cargo configuration similar to that used in the all-cargo configuration. The cargo compartment in the passenger-cargo configuration is ventilated down through the cabin floor forward into the lower avionics area.” This line is also not explained, and doesn’t reflect what I read in the operations manual, but the manual was from a different airline and might not have matched 1:1 to the configuration used by Pan Am.
The above quote appears to refer to a 707 “combi” configuration where the main deck is divided into a cargo area in the front and a passenger area in the rear. In an all-passenger configuration, air in the cabin flows toward the rear and out the rear outflow valve, but in a combi format, one would not want smoke from a fire in the cargo area to flow aft into the passenger area, so it makes sense that an alternate route would be established to ventilate the cargo area downward through the lower 41 and out the forward outflow valve instead. The above quotation also shows that this vent configuration was used on cargo-only versions of the 707–320C, which could include the accident aircraft.
From the above information, I would hazard a guess that the smoke chute was intended to evacuate smoke from the main deck overboard via the lower 41 avionics compartment. This would also explain the references to a “barrier,” as such a chute would form part of a smoke barrier system designed to keep smoke out of occupied areas. But while this is one plausible interpretation of the information in the report, I’m still not 100% certain that it’s correct.
Regardless of the answer, it remains true that as the fire spread through the main cargo deck on Pan Am flight 160, smoke made its way into the lower 41, where it was seen by the crew through the pressure relief vent prior to any formal indications from the smoke detectors. We know that if the main deck smoke detectors had illuminated first, then the crew probably wouldn’t have reported that the lower 41 was the source of the smoke. They also might have suspected that the smoke came from the main deck if they had been properly notified of the nature and quantity of the hazmat on board. But because neither of those things happened, they quickly developed an incorrect mental model of where the fire was located.
The fact that the crew believed the smoke was coming from the avionics compartment turned out to be crucial to the sequence of events. If electronic equipment in the lower 41 was overheating or malfunctioning, then the source of smoke could be identified, isolated, and eliminated. But if there was a fire burning in the main cargo deck, there was little the crew could do about it, and there would be a correspondingly higher level of urgency.
In their initial communications, the level of urgency displayed by the crew was rather low. At first, Captain Zammett and First Officer Ritter discussed the possibility of flying all the way back to New York, which would not be a reasonable course of action if they believed they were in an emergency. Zammett also said to Flight Engineer Melvin, “You don’t think you could get down there and spot that, huh,” suggesting that he climb into the lower 41 and try to figure out what was burning.
“I can’t get around down there at all, I — I don’t see any reason why that ####*, it should’ve popped a breaker by now. It ought to short out somewhere,” said Melvin. In his opinion, electrical smoke in the avionics bay should be associated with a tripped circuit breaker, which was an apt assessment. Unfortunately, this evidence didn’t cause the crew to question whether the fire was actually in the lower 41 — a classic form of psychological bias.
*In the CVR transcript, the # symbol represents an expletive that was redacted. In previous articles, I sometimes attempted to guess what expletive was used based on context in order to make the text flow better. However, I’ve decided not to do this anymore.
First Officer Ritter now jumped in with a suggestion. “Can we increase our airflow so we get rid of some of the smoke through the outflow valves and equipment cooling circuit?”
“Yeah,” someone said.
“Just stick your head down there and see if it’s still coming,” Captain Zammett suggested to the flight engineer.
At 09:06, the Boston air traffic control center, still unaware of the situation, instructed flight 160 to contact Montreal center as the aircraft crossed the border into Canada. Seconds later, Pan Am operations stated that they would prefer the flight to return to New York, as opposed to Boston.
As First Officer Ritter worked out their turn back to New York with Boston and Montreal, Flight Engineer Melvin continued to watch the smoke drifting up into the cockpit from the floor vent. “This # sure is coming, John,” he said to the captain. “Lemme see if I can shut this, ah, blower off. I’m gonna raise the cabin up — up to ten thousand?”
Melvin’ appeared to be following the emergency Smoke Evacuation procedure, on which the second item, after optionally donning oxygen masks, was to reduce the cabin pressure to the equivalent of 10,000 feet altitude. This would cause air to flow out of the cabin and cockpit faster, hopefully reducing the smoke.
“Try that,” said Captain Zammett.
“Could open a bleed and try to get some air in this ####,” Melvin added, referring to the next item on the checklist, which was to set the bleed valves to “maximum on” in order to increase airflow into the cabin and cockpit. This action would complement the previous step, which was to increase airflow out.
“Go ahead,” said Zammett.
On the radio, First Officer Ritter finally established contact with Montreal and stated their intention to return to New York. “Turn right heading one eight zero,” Montreal replied.
In the cockpit, the smoke wasn’t going away. “It’s still getting thicker, isn’t it?” Zammett asked.
“Seems like there could be equipment…” Melvin started to say.
“There is no smoke in those detectors though, is there?” Zammett asked.
“Well, there is now,” said Melvin. Apparently enough smoke had finally reached the main deck smoke detection windows to give him an indication.
“There is?” said Zammett.
“Yeah.”
“Where would that pick it up from?” Zammett wondered. “Back there, or…?”
“Well, it’s probably going up this way and coming back around,” Melvin said, suggesting that the smoke in the main deck must have come from the lower 41 via the cockpit. In fact, it was the other way around, and this statement marked another example of confirmation bias at work.
“Turn the equipment cooling blower off,” Melvin said. “I think you don’t need to go in the back then.” Normally, a main deck smoke indication would prompt one of the pilots to check the main deck, but since they had convinced themselves they already knew the source of the smoke, they decided not to.
“Right,” said Zammett.
“Because it should pop a breaker someplace,” said Melvin.
“Yeah.”
“We ought to go on oxygen, this #’s getting a little thick, eh?” Melvin added.
Before the crew could act on that suggestion, Zammett called Pan Am Operations to report that they were heading back to New York and that the smoke was getting thicker. Operations asked if they needed equipment on arrival, to which Zammett told them they would make that decision in a few minutes.

At this time, flight 160 completed a 180-degree turn overhead Sherbrooke, Quebec, and was now proceeding back into the United States. First Officer Ritter signed off with Montreal and returned to Boston Center.
“##, it is getting heavy,” Zammett exclaimed.
“I think we better take it to Boston,” said Melvin.
“Yeah.”
“This # is getting thick back here,” Melvin repeated.
Diverting to Boston was faster than going to JFK, but it still wasn’t the closest airport. If the crew believed they were in an emergency, they would probably have diverted to Montreal. However, Boston was the nearest airport with a Pan Am maintenance facility, which suggested that they believed this was a problem that could be managed in the air and fixed on the ground.
As First Officer Ritter called up Pan Am Operations again, Captain Zammett said, “Tell ’em we wanna get down and head for Boston.”
“Yes sir, I think we’re gonna take this thing into Boston, this smoke is getting too thick,” Ritter reported to Operations.
Moments later, at time 09:11, all three crewmembers donned their oxygen masks, and then First Officer Ritter called for the descent checklist and requested descent from Boston center. The center then cleared them to descend from 31,000 to 19,000 feet.
“Do you guys want to get your goggles?” Zammett asked, referring to the smoke goggles, which they promptly put on.
Over the radio, Pan Am Operations asked, “Are you requesting equipment on arrival at Boston sir?” In this case “equipment” refers to the fire trucks.
“Do you want equipment on arrival at Boston?” Melvin asked. “Probably wouldn’t hurt, huh?”
“Stand by one — I don’t know, what did — how’s the smoke doing?” said Zammett.
“That #### is full back there,” said Melvin. He was probably looking into the crew rest area behind the cockpit, which was starting to fill up as smoke seeped through the barrier separating it from the main deck. Later tests proved that this barrier was somewhat permeable if the smoke was thick and/or if the curtain was poorly maintained.
“Better have the equipment,” Zammett concluded. In response, Melvin requested that Operations notify Boston to roll the fire trucks.
The pilots now began the descent checklist and grabbed their approach charts for Boston. First Officer Ritter also notified Boston of the nature of their emergency — although it was Boston who used the term “emergency,” not flight 160.
By 14:14, the transcript makes clear that the seriousness of the situation was increasing. At that time, Boston asked flight 160 to change to a new frequency, but Ritter requested to remain on their current frequency because “It’s too # hard to change.” Most likely he was unable to see the radio clearly enough due to the heavy smoke. This issue would have been even worse for Captain Zammett, whose smoke goggles didn’t fit properly over his spectacles, leaving gaps around the edges that allowed smoke inside. Modern smoke goggles don’t have this issue, but the goggles on the 707 were extremely primitive.
Flight 160 was now cleared direct to Boston, descending over Maine. With growing concern, Zammett asked the flight engineer, “How does it look in the back, Dave?”
“It’s full,” Melvin replied.
“Smoke detector showing much?”
“No, ah, it’s showing the same as it was,” said Melvin. “We’re somehow getting it up through the floor from down below and it’s going in the back I think.”
The pilots had no idea that inside the main deck, a raging fire was consuming a pallet of caustic chemicals located just aft of the wings.
At this point, Melvin suddenly realized that they were over their maximum landing weight. “We weigh 278 [thousand pounds] right now,” he pointed out.
“Okay, I think we’ll take it on in,” Zammett said, expressing his intention to land without delay despite their high weight.
“Just ease it on, it should be okay,” Melvin agreed.
Hopping on the radio, Zammett told Boston, “We’d like to get down as soon as possible so we can burn off some fuel rather than dump.” By flying at a lower altitude the rest of the way to Boston, they would burn fuel less efficiently, reducing the weight of the airplane at landing.
Meanwhile, Melvin continued to examine his panel for any sign of a problem, but there was nothing. “I can’t find a thing wrong back here,” he said. All systems were working normally.
“Okay, uh, maybe it’s in a package,” Zammett suggested.
“Could be,” said Melvin.
“Ah, you didn’t get in to open the door into the back section, did you?” Zammett asked. It seemed as though the pilots were on the brink of a realization. If they had been informed that there was hazmat on board, they would certainly have taken the possibility seriously. But instead Zammett said, “Ah, they’re supposed to be flame resistant or fire resistant anyhow, isn’t it?”
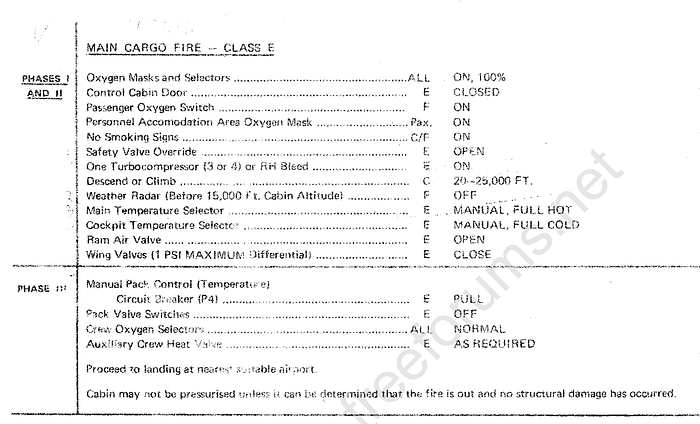
The main deck cargo hold was what’s known as a Class E compartment. The primary method of controlling a fire in a Class E cargo compartment is to depressurize the aircraft to starve the fire of oxygen. However, the pilots of flight 160 never attempted to do this, and even if they had, it wouldn’t have worked, because the reaction between the nitric acid and sawdust was generating its own oxygen. This comment therefore represented a misunderstanding of the nature of both the fire and the 707 itself.
“Well, I — I looked back there — the smoke — there’s more smoke back there, but there’s none up here now,” said Melvin. As the heat of the fire cracked more nitric acid bottles, the amount of smoke would periodically increase, only to subside again temporarily before the next box of acid became involved, creating the fluctuations observed by the flight engineer. But, concluding his thoughts, Melvin again stated, “It must — it’s in the lower 41 someplace.”
“I think so,” Zammett agreed. It was an assumption that would seal their fate.
Over the next few minutes, Zammett continued to speak intermittently with air traffic control while discussing their plans with Melvin. They resolved to make a normal landing using the normal checklists, but Melvin also suggested that they advise the fire department of the suspected electrical fire. Zammett also decided that they would land on runway 33 because it was longer and the airplane was heavy. Later, Melvin informed Pan Am Operations that the fire was “either in the lower 41 or the forward cargo hold” but that “there isn’t too much [smoke] in the cockpit right now.”
Descending toward 2,000 feet, the pilots set up their instruments to capture the instrument landing system for runway 33 and completed the approach checklist. Zammett also instructed, “Ah throw the gear down please,” presumably to increase drag and use more fuel.
“Gear coming dow — “ First Officer Ritter started to say.
“Hold it, hold it,” Zammett interrupted. “Wait till I slow it down, we’ll tear the # doors off.” Due to their lengthy descent, their airspeed was too high to safely deploy the landing gear.
Meanwhile, Melvin was speaking with Operations. “Clipper 160, if you’re on the freq, would you advise us if the lower motor CB has been pulled, the blower motor CB,” Operations said, referring to the circuit breaker for the electronics equipment cooling blower. It’s not entirely clear why Operations would suggest this, given that the blower forces air into the lower 41 from the cockpit, and thus presumably was helping to keep the smoke out.
“I tried that, it didn’t make any difference,” Melvin replied.
Finishing up the checklist, Zammett commented, “I don’t smell that smoke as much now, there doesn’t seem to be as much, does it?”
“Ah, it doesn’t seem to be as much,” Melvin agreed. He then called the engineer’s check and approach check complete; all that remained was the landing checklist. But just moments later, at time 09:29, he suddenly said, “Ah, it’s definitely coming out of lower 41.”
“Still coming out, huh?” Zammett asked.
“Yeah,” said Melvin. “That’s worse, I don’t see — ”
In the background, Boston center reported that they were 45 miles from the field.
“It’s getting worse?” Zammett asked.
“Ah, I turned the equipment blower off and that made it worse,” Melvin explained. This was an expected result for the reasons I stated above. In fact, airflow testing later proved that the blower was practically the only thing keeping them alive. Without it, smoke would flow from the lower 41, through the pressure relief vent, and into the cockpit completely unimpeded.
“Okay, then if that’ll blow it out if you take the — keep it moving won’t it?” Zammett said.
“Yeah, I just pulled the breaker out again. I tried the CB to see if that’d do it but the — ” Melvin said. “Okay, it’s, uh — “
“All of a sudden it’s getting worse in here,” Zammett interrupted.
“It’s somewhere down in lower 41,” Melvin repeated once again. He then pushed the breaker back in to restart the blower.
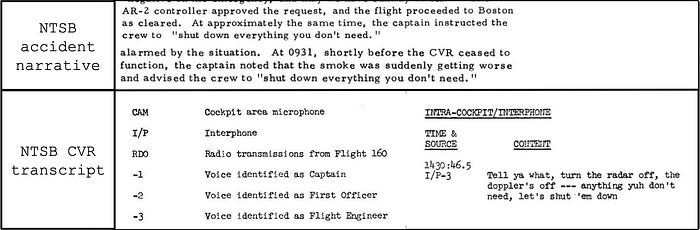
At this point a critical event occurred, but the NTSB report’s discussion of it contains a confusing contradiction. According to the narrative in the NTSB report, at approximately 09:31 Captain Zammett instructed the crew to “shut down everything you don’t need,” with quotations, implying a direct quote from the cockpit voice recording. However, the CVR transcript shows that at time 09:30:46, a person identified as the flight engineer, stated, “Tell ya what, turn the radar off, the dopplers off — anything ya don’t need, let’s shut ’em down.” At no point in the transcript does Captain Zammett issue an instruction similar to this, nor does anyone use the exact words quoted in the NTSB narrative. In fact, Zammett never even acknowledges Melvin’s desire to start turning off unnecessary systems.
It follows from this discrepancy that either the NTSB’s analysis of the accident or the CVR transcript misattributes and misquotes this crucial statement. Even after researching this accident in considerable depth, I’m still not sure who actually said it.
Whichever crewmember it was, they evidently wanted to shut down nonessential systems in an effort to isolate the source of the smoke. With no popped circuit breakers on his panel and no failure indications from any systems, yet having convinced himself that the smoke was coming from the avionics compartment, there was little left for the flight engineer to do except start turning things off just to see if it made any difference.
The first thing Melvin turned off was the weather radar, which was not needed since there was no significant weather in the area. “That’s off,” he announced. “Okay, it’s VFR, could I turn the ah, radio altimeter off?” The radio altimeter was most useful during instrument flight conditions; under visual flight rules, or VFR, he felt they wouldn’t need it.
Melvin never received a reply to these statements. At that time, First Officer Ritter was engaged in continuous conversation with Boston ATC, who told them to expect a visual approach to runway 33 left. The controller also asked if they were declaring an emergency, to which Ritter replied, “negative.” Ritter and Zammett then spent around 30 seconds discussing their landing weight.
After a awhile, Melvin interrupted to say, “Doesn’t seem to be getting any worse.”
“No, but I don’t think it’s getting any better, is it?” Zammett replied.
“No, it’s not getting any better,” Melvin agreed.
“It’s getting worse right now, you can see it blowing around here,” Ritter added.
Without further discussion, the pilots launched into the landing checklist. Boston ATC began vectoring them for a five mile final approach. Moments later, at 09:34:56, the cockpit voice recording ended mid-flight.
◊◊◊
By the time flight 160 was maneuvering for final approach, the fire in the main deck cargo area was burning ferociously both above and below the floor level, reaching temperatures in excess of 1,000˚F (538˚C). Evidence indicates that the fuselage skin adjacent to the fire started to melt while the plane was still in the air. The fire is also thought to have destroyed the wires that powered the cockpit voice recorder, resulting in its premature shutdown.
Thanks to various clues, some information is known about what happened during the final five minutes of the flight after the end of the CVR. For instance, based on the recovered positions of switches on the flight engineer’s panel, it was apparent that after turning off nonessential systems, flight engineer Melvin began working through the “Electrical smoke or fire” emergency checklist, pictured below. Since the origin of the smoke was not electrical in nature, none of the suggested solutions would have worked, and he would have progressed quite far down the checklist. One of these later steps was to set the “essential power” switch to “external.”
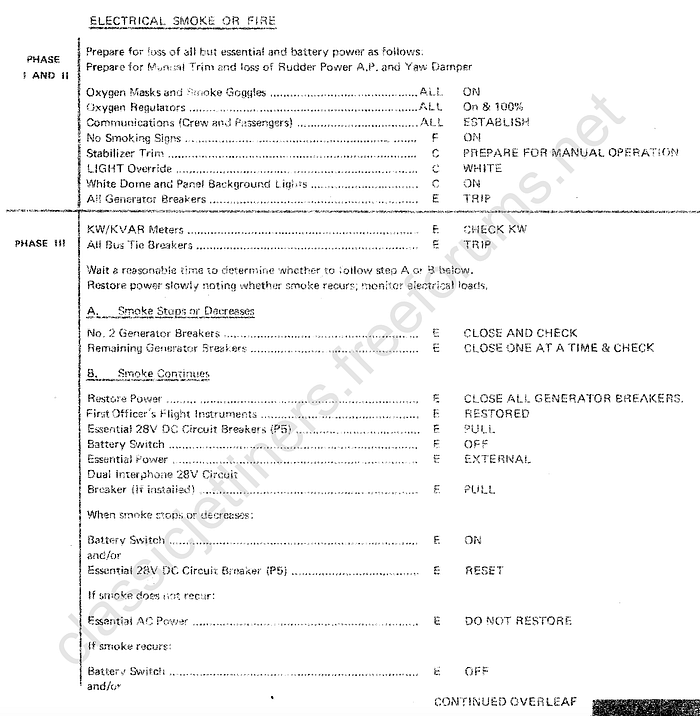
The essential power switch affects the power source for all systems on the “essential bus,” which distributes electrical power only to the most crucial systems on the airplane — as the name implies. To get this far in the checklist, you have to try turning off damn near everything else first, without success.
Setting the “essential power” switch to “external” will configure the essential bus to distribute power from an external power source when the aircraft is on the ground. In the air, since there is no external power source, this position cuts power to the bus and all systems on it. Those systems would have included the captain’s instrument panel, the captain’s VHF radio, the cockpit voice recorder, the transponder, the cockpit interphone system, and the yaw damper, among other items. However, by this point the CVR had already failed.
After the accident, the essential power switch was indeed found set to “external,” indicating that Melvin must have cut power to essential systems at some point after the end of the CVR recording. It’s not known whether the crew followed the advice at the start of the checklist, which advises the pilots to “prepare for manual trim and loss of rudder power A.P. and yaw damper.” In fact, the NTSB suspected that such preparations were not made.
As flight 160 aligned with the runway and commenced its final approach, the controller asked, “Clipper 160, advise anytime you have airport in sight.” But there was no reply from the aircraft. Seconds later, its transponder disappeared from the controller’s radar screens, although the airplane was visible in the distance, clearly still airborne. The loss of radar and radio contact were actually caused by the loss of the №1 VHF radio and transponder when the flight engineer cut power to the essential bus.
If the pilots were properly preparing for each step, they would have moved the VHF radio selector switch to №2, allowing both pilots to use the still-powered alternate VHF radio. However, the loss of radio contact, and the crew’s failure to reestablish it, suggests that the flight engineer cut essential power without ensuring that the other crewmembers understood what would happen.
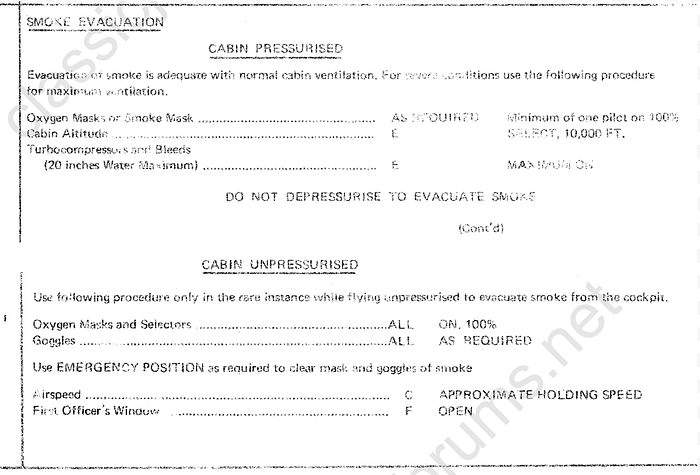
This breakdown in crew communication might have taken place amid rapidly deteriorating conditions inside the cockpit. Witnesses on the ground reported that during the last phase of the approach, smoke was pouring through the open left cockpit sliding window. Thick smoke deposits were later found around this window, testifying to extreme conditions inside. Most likely, amid thickening smoke, the pilots opened the window in accordance with the final, most desperate solution prescribed by the cockpit smoke evacuation checklist. Unfortunately, the checklist assumed, first of all, that the smoke source was inside the cockpit; and second, that smoke was not being generated continuously. Neither of those was true in this case, and in fact, opening the cockpit window while a fire is actively burning inside the main deck cargo area was experimentally demonstrated to increase the rate of smoke intrusion into the cockpit. Considering the captain’s poorly fitting smoke goggles, and the fact that cutting essential power disabled the interphone that the pilots were using to communicate through their oxygen masks, their ability to fly the airplane would have been substantially compromised from that point onward.
But in the end, the real killer wasn’t the smoke: it was the inoperative yaw damper. And to explain why, we need to go down yet another, no less fascinating rabbit hole.
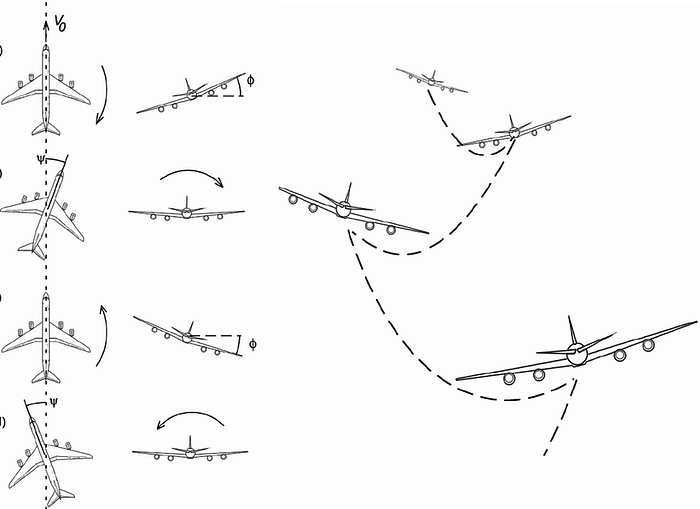
The yaw damper is a device that automatically makes constant, small rudder inputs in order to prevent unwanted excursions on the yaw axis — that is, nose left and nose right. All large swept wing jets have a yaw damper to improve their directional stability, and in fact the 707 was one of the first aircraft to incorporate one.
Without a yaw damper, swept wing jets tend to fall into a dynamic cycle known as “Dutch roll.” Basically, as the plane starts to yaw in a particular direction, let’s say nose right, then the left wing moves into a position where the airflow over its surface is more direct, resulting in increased lift. At the same time, the right wing falls back into a less advantageous position, resulting in decreased lift. Then, with more lift on the left and less on the right, the airplane starts to roll to the right. So in other words, a yaw tends to turn into a roll in the same direction. But as the yaw, or sideslip angle, increases, the aerodynamic force against the big, flat side of the vertical stabilizer also increases, until eventually that force causes the entire aircraft to weathercock back the other way. The yaw angle then passes back through neutral and into the opposite position, which in our example would be nose left. Correspondingly, the direction of bank reverses from right wing down to left wing down. This cycle then repeats, over and over and over — and that’s what we call Dutch roll.
Dutch roll is typically excited by a sudden yawing force, such as a lateral wind gust or an accidental rudder input. It’s not inherently dangerous on most aircraft but it is extremely uncomfortable for the occupants, so the yaw damper works constantly in the background to ensure that it doesn’t happen. And even if it does, the pilot can recover simply by holding the wings level.
Even without the yaw damper, modern aircraft are designed so that their inherent Dutch roll characteristics are either stable (the amplitude of each swing is smaller than the one before it) or neutral (the amplitude of each swing is equal to the one before it). This is as opposed to an aircraft with unstable Dutch roll characteristics, in which each swing is larger than the one before it, which will eventually result in either loss of control or in-flight breakup of the aircraft if not corrected by the pilot or the yaw damper.
Because the 707 was one of the first jet airliners ever designed, its engineers were not as successful at damping its Dutch roll characteristics as they are today. Early 707s were inherently unstable in Dutch roll without the yaw damper under all conditions. In later versions, this tendency was reduced, but some edge cases remained. Dutch roll on any aircraft is worse at low speed and high angles of attack with the flaps extended simply because these factors reduce controllability on the roll axis (i.e., larger inputs on the flight controls are required to produce the same roll response). This tendency is made even worse if the pilots have extended the speed brakes to reduce lift and slow the plane for landing.

According to the NTSB, flight testing has demonstrated that with the flaps fully extended to 40 degrees, the speed brakes extended, and the yaw damper inoperative, the Boeing 707’s Dutch roll characteristics become so unstable that “lateral control capability may be extremely limited, if not impossible.” In other words, the roll inputs required to recover from Dutch roll in that configuration equal or exceed the limits of the pilot’s roll authority.
Before Flight Engineer Melvin started turning off critical systems, the pilots had not successfully stabilized the airplane for landing. In fact, when they made the final turn onto their truncated final approach, the aircraft was too high and was traveling too fast, which prompted the pilots to extend the flaps to 40 degrees and deploy the speed brakes in an attempt to slow down. Subsequently, when Melvin cut power to the essential bus, the yaw damper was disabled, placing the airplane into a configuration in which it was uncontrollable. If this matter had been discussed with the pilots beforehand, it’s doubtful that Melvin would have proceeded with cutting power, so it’s almost certain that Captain Zammett didn’t know that this was about to happen.
On the ground, witnesses watched with growing alarm as the aircraft started to sway from side to side, back and forth, over and over, each swing growing larger and wilder than the one before. The aircraft was experiencing unstable Dutch roll, and although the pilots no doubt fought to halt the exaggerated gyrations, the only way to save the plane was to turn the yaw damper back on. Unfortunately, amid the chaos, the flight engineer never managed to do so.
Moments later, at approximately time 09:40, the airplane entered a bank that was too steep to sustain; the wings lost lift, the nose fell through, and the 707 dived toward the ground. Within a few seconds it was all over. Pan Am flight 160 spun and impacted the ground next to the threshold of runway 33, traveling almost perpendicular to the runway, in a steep nose down attitude with nearly 90 degrees of left bank. The fuel tanks exploded on impact, sending a huge fireball curling over Logan Airport as burning debris careened across the threshold, over the seawall, and into Boston harbor, setting fire to the approach lighting pier. Firefighters rushed to the scene and quickly extinguished the fire, but their rescue efforts were fruitless; all three crewmembers died on impact.
◊◊◊
The National Transportation Safety Board’s analysis of the events leading up to the crash of flight 160 focused on three principal areas: the design of the aircraft; the actions of the crew; and the packaging and loading of the hazmat.
Although readers’ attention with regard to aircraft design is probably drawn toward the instability of the 707 in Dutch roll, this matter only received a single line in the NTSB report, and I had to do considerable outside research to confirm what the actual problem was. Instead, most of the NTSB’s focus was directed at the means available to exclude smoke from the cockpit. After all, the smoke in the cockpit was the motivating factor that led the crew to start searching for increasingly dangerous solutions. It also probably compromised the crew’s ability to fly the airplane safely during the final minutes due to lack of visibility.
Under federal regulations at the time, and still today, a class E cargo compartment, such as the main deck of a purpose-built freighter, must have “means to exclude hazardous quantities of smoke, flames, or noxious gases from the flight compartment.” If that regulation sounds familiar, then you’re probably thinking of my previous article on UPS Airlines flight 6.

To recap that story, in 2010 a Boeing 747 freighter experienced a fire in the main cargo deck, a class E compartment, due to thermal runaway of improperly packaged lithium batteries. The 747’s air conditioning packs were supposed to maintain positive pressure between the cockpit and the main deck so as to exclude smoke from the crew area. However, the procedure for extinguishing a fire in the main deck was to depressurize the hold, which involved turning off two of the three air conditioning packs. Not only did this fail to extinguish the fire, which was fueled by a chemical reaction that didn’t need oxygen to sustain itself, it also left the crew with no smoke protection after the third and final air conditioning pack suffered an unrelated malfunction. The cockpit subsequently filled with smoke, leading to the incapacitation of the captain. The first officer attempted to land the plane by himself but he was unsuccessful due to being unable to see.
In that accident, the United Arab Emirates General Civil Aviation Authority, which led the investigation, determined that the concept of a class E cargo compartment was potentially flawed, in that depressurizing the compartment required maintaining a high altitude to starve the fire of oxygen, which was in conflict with the need to land immediately in the event of a fire. They also found that depressurizing the hold was ineffective against fires involving hazardous materials and possibly ineffective against normal fires as well. Furthermore, the smoke detection systems wouldn’t detect the fire early enough to intervene before it became catastrophic if the fire started inside a container or a pallet with a rain cover. Investigators also expressed concern that the design of the 747’s emergency checklists did not provide adequate assurance that smoke would not enter the crew area.
If all of this sounds like it should apply to Pan Am flight 160 as well, that’s because it does. The procedure for a fire in the class E compartment on the 707 was also to depressurize and climb to a high altitude, which would have failed to extinguish the fire on flight 160 because nitric acid is an oxidizer that produces its own oxygen. This issue was tangentially addressed in the NTSB report, although the report didn’t discuss the inherent contradiction between this directive and the need to land immediately, even though investigators noted that the pilots should have landed immediately if they knew there was hazmat on board. Additionally, as in UPS 6, the smoke detector failed to provide timely warning of the fire, contributing to the pilots’ erroneous assumption about the location of the blaze.
Once the fire was underway, the smoke barrier between the main deck and the crew area generally prevented smoke from entering the cockpit in a wholesale manner, but based on the pilots’ statements, considerable smoke nevertheless made it into the cockpit by traveling down the smoke chute from the main deck, into the lower 41 compartment, and then up into the cockpit via the pressure relief vent. The NTSB and the FAA were concerned that this had happened even though the pilots followed the smoke evacuation checklist by increasing the cabin altitude to 10,000 feet, opening the outflow valves, and turning the bleeds to max. The exact reason why these actions failed to prevent smoke intrusion wasn’t determined, but investigators believed that the existence of an alternate airflow path into the cockpit via the lower 41 caused the 707 to fall short of the regulatory requirement for “means to exclude hazardous quantities of smoke… from the flight compartment.”
After the accident, testing also showed that thick smoke would rapidly enter the cockpit via this route if the equipment cooling blower was turned off. This didn’t cause the smoke intrusion on flight 160 even though the flight engineer turned the blower off twice, simply because he turned it back on right away. But the FAA was concerned that if an electrical problem were to occur, or the blower malfunctioned, then there would be nothing to stop smoke from freely entering the cockpit. Doesn’t that sound a lot like what happened on UPS flight 6, with its malfunctioning air conditioning pack?
In 1974, the FAA laid out some of these concerns in a letter addressed to Boeing, which cited the Pan Am flight 160 CVR transcript to argue that the pilots followed the smoke evacuation procedure but that the procedure was ineffective. However, Boeing replied that it had conducted smoke generation and airflow tests in May 1974 and found that the procedures adequately excluded smoke. Even when a continuous smoke source was placed in the main deck, Boeing reported that smoke didn’t move from the lower 41 into the cockpit. Boeing also argued that the CVR didn’t contain sufficient evidence to conclude that the pilots had followed the procedures correctly.
However, in their reply to the FAA, Boeing also wrote, “If the procedure is followed, a continuous source of smoke will not exist as the fire will be smothered, except in the rare case where a hazardous material is carried which is packaged and handled such that it is released, generates heat, and provides its own oxygen.” So in other words, exactly what happened on Pan Am flight 160 and UPS flight 6 — and on several other notable flights, including but certainly not limited to ValuJet flight 592 (1996, 109 killed), American Airlines flight 132 (1988, 13 seriously injured), and Asiana Airlines flight 991 (2011, 2 killed). All of these accidents and incidents involved fires caused by hazardous materials that generated oxygen as a byproduct, allowing them to grow and expand inside a cargo compartment where the active means of fire suppression was oxygen starvation, including compartments designated both class E and the now-defunct class D. So while it’s true that such accidents are rare, they aren’t really as rare as Boeing wanted to believe. Boeing also didn’t explore the possibility that depressurization is not fully effective at stopping non-self-oxygenating fires, which we know today to be true.
One of the big issues with Boeing’s mindset was that checklists related to smoke clearance assumed the fire was already extinguished, which could cause the pilots to take potentially dangerous actions if smoke was still being generated. In fact, there are many reasons why a crew might not be able to extinguish a fire, including not only the reasons discussed above, but also other reasons, such as incorrect identification of its source (e.g. Pan Am flight 160); a fire in an inaccessible location (e.g. Swissair flight 111, Air Canada flight 797); or a fire whose intensity exceeds the capabilities of the available extinguishing equipment (e.g. South African Airways flight 295). In any of these situations, the crew might — and in several of the above cases, actually did — attempt to evacuate smoke while the fire was still burning.
If the flight crew reaches the final step on the smoke evacuation checklist, they will be advised to open a window in flight. On the 707, this was the cockpit sliding window; on UPS flight 6, this was a specially designed smoke shutter in the ceiling. But already in 1973, it had been demonstrated that opening a window in the cockpit while the fire is still burning will create an airflow path that draws more smoke into the cockpit. Despite this, the checklist didn’t warn the crew to apply the procedure only after extinguishing the fire. In fact, this warning also wasn’t included in the smoke and fumes removal checklist used by the ill-fated UPS crew 37 years later, and consequently that crew also unknowingly worsened the smoke intrusion by opening the smoke shutter. It’s unclear that either accident would have been prevented if the crew had kept the windows closed, but opening them certainly didn’t help.
In its final report, the NTSB recommended that the design of the 707 be changed to exclude an airflow path that could cause hazardous quantities of smoke to enter the cockpit; that operators be provided with supporting data to create more effective smoke evacuation procedures; and that the FAA evaluate whether certification tests adequately reflected the range of situations in which flight crews would apply the smoke evacuation procedures. Unfortunately, the NTSB did not specifically recommend that Boeing and the FAA reevaluate the checklist instruction to open a window, or the assumption that it’s possible to extinguish a fire in a class E cargo compartment by depressurizing the airplane.
The NTSB also recommended that flight crews receive more training on how to identify the source of smoke or fire, and that flight crews be trained to land immediately following any in-flight occurrence that they believe to be related to hazmat on board the aircraft. But while these recommendations seemed sensible at the time, modern guidance for flight crews is to land immediately whenever smoke or fire is present, regardless of what the pilots believe is the source. In several accidents during the 1970s and 1980s, including flight 160, flight crews facing in-flight fires did not land at the nearest available airport because they falsely believed that the fire was in a location that did not directly threaten the safety of the airplane. Encouraging identification of the source of unknown smoke before making a decision about whether to land immediately was an industry practice that cost lives. Identifying the source is still important, but it must come after the decision to land.
In my opinion, Pan Am flight 160 represented a missed opportunity to reevaluate the assumption that flight crew identification of the smoke source was an appropriate or reliable means by which to judge the severity of a fire emergency.
◊◊◊

The second major issue that contributed to the accident, after aircraft design, was crew coordination. Most significantly, the pilots might have been able to land the plane in one piece if the flight engineer had not cut essential electrical power, disabling the yaw damper. The flight engineer’s decision to follow the provisions of the “electrical fire or smoke” checklist was not coordinated with the pilots and the crew apparently did not discuss or prepare for the effects of shutting off essential power. Modern crew resource management training emphasizes the role of each crewmember in maintaining group awareness through the use of callouts and collective decision-making. But in 1973, this training did not yet exist, nor did the investigators conceive of its future importance, and no recommendations related to the issue were made.
The misidentification of the smoke source also highlights the dangers of confirmation bias. At several points during the emergency, the flight crew considered the possibility that the fire might be on the main deck, and even named multiple indications that the fire was not in the avionics compartment, including the absence of any popped circuit breakers or equipment malfunction warning lights. And yet, despite these doubts, no crewmember ever went to the main deck to check whether the cargo was the source of the fire. Instead, they repeatedly rationalized their initial incorrect assumption despite growing evidence that it was wrong. This is a natural human tendency that has to be actively resisted using error entrapment and mitigation strategies — strategies that are taught today, but were not taught in 1973. If the crew had been taught how to constantly reevaluate their mental models of the situation based on the raw indications that they were receiving, they might have decided to check for a fire on the main deck — and if they had done that, the flight engineer wouldn’t have started turning off electrical equipment, and the crash might not have happened.
◊◊◊

The third major causal factor was the failure by multiple companies to ensure that the nitric acid shipment was properly packaged and loaded. Based on my analysis of the information in the NTSB report, Allied Chemicals most likely packaged the nitric acid bottles with flammable sawdust cushioning; Santini Brothers, entrusted by NSC to repackage the acid for air transport, did not replace the sawdust or affix the required warning labels; and Pan Am’s cargo loaders turned the boxes of hazmat sideways in order to fit them into the aircraft. Each of these mistakes contributed directly to the eventual leakage and fire that brought down the plane.
Given the number of people and companies involved in this chain of errors, it was impossible to assign blame to any single person or entity. Legally speaking, regulations at the time placed responsibility for proper hazmat packaging onto the shipper, who in this case was NSC, but NSC had no operational control of the shipment at any point before it was loaded onto the aircraft. In fact, NSC was not involved in the shipping business and had no means whatsoever to ensure proper handling of the materials. Instead, the nitric acid was packaged and transported by employees of ACC, Santini, P. Calahan Inc., and Pan Am’s contract cargo agent Interamerican. Among the people at these companies who directly handled the nitric acid, the only person with any recent or formal hazmat training was the Santini office manager, and even he accepted Lyon’s assertion that sawdust was a safe cushioning material for an oxidizing chemical.
Part of the problem was that regulations surrounding hazmat handling, packaging, and transport are extremely complex with detailed requirements for each individual chemical. It was difficult even for trained personnel to become familiar with all the requirements, and the US Department of Transport had not published any single document containing all of the relevant regulations. As a result, even in cases where personnel received hazmat training, it wasn’t particularly easy to access the rules that they were expected to follow.

Today, FAA and DOT hazmat rules can be found on the internet by consulting the US government’s electronic code of federal regulations, Title 49, Subtitle B, Chapter I, Subchapter C, Parts 171–180. As an experiment, I — a complete amateur with no hazmat training and no previous experience with these regulations — decided to see whether I could figure out how to transport nitric acid by air in 2025. In the end, it took several hours for me to learn how to navigate the system of tables and codes linking each part of Subchapter C, but I was eventually able to determine that nitric acid with a concentration below 70% can be carried on cargo aircraft in bottles not larger than 2.5 L; the bottles must be glass, earthenware, or plastic with a metal overpackage; for bulk carriage, the bottles must be placed into an aluminum or steel canister; and the canisters must be placed into wood or metal boxes of certain federal specifications. I wasn’t able to find any requirements for a cushioning material that applied to nitric acid, however I did find cushioning material standards with codes applying to certain other chemicals. I’m still not entirely sure whether regulations no longer require noncombustible cushioning material, or if I just missed something due to inexperience. The regulation specifying the cushioning material that was quoted in the NTSB report, Part 173.268, no longer exists. So if I were to follow the regulations I found to the letter — not that I would ever do this, seeing as I’m not qualified to ship acid — then I would have put the nitric acid into 2.5 L glass bottles, put the bottles into metal canisters, and then put the bottles into DOT specification boxes with labels reading “corrosive” and “oxidizer.” I didn’t find where the regulations require “this end up” labels, but I’m sure they do somewhere.
Using this tool, and assuming I had access to the proper containers, I would have packaged the nitric acid more safely than it was packaged for Pan Am flight 160. Due to my lack of training and unfamiliarity with the system, I would have made some mistakes, but probably not as many. So the conclusion I’ve drawn from this exercise is that US hazmat regulations are vastly more user-friendly today than they were in 1973, even though they remain extraordinarily complicated. Furthermore, the availability of hazmat training is much more widespread than it was in 1973, and most employees involved in handling hazmat today are required to receive formal training.

Although a lot of this improvement has to do with the miraculous invention of the internet, awareness and enforcement of hazmat regulations also improved as a result of several NTSB recommendations stemming from Pan Am flight 160. These recommendations included the following:
- The FAA should make the dispatcher directly responsible for notifying the captain of the presence of hazardous materials in the cargo.
- The FAA should prohibit air carriers from relying on the shipper’s word as prima facie evidence of the shipment’s compliance with hazmat regulations, and require air carriers to implement a system for inspecting hazmat shipments at the receiving point prior to loading them onto an aircraft.
- The FAA should create a system for air carriers to notify the FAA if a shipment is found not to be in compliance with hazmat regulations, and require the use of this system.
- The FAA should conduct a one-time inspection of each air carrier’s cargo receiving, palletizing, inspecting, and loading procedures to ensure regulatory compliance.
- The FAA and DOT should develop a checklist that personnel can use to determine whether a hazmat shipment meets federal regulations.
- The FAA should disseminate information about the requirements for air transport of hazmat directly to air carriers’ sales’ representatives who accept bookings from shippers.
The FAA ultimately implemented almost all of these recommendations. In addition to improving access to hazmat information, these changes also motivated air carriers to inspect and handle hazmat more cautiously, as regulations now hold carriers partly responsible for the safe packaging of hazmat carried aboard their aircraft.
◊◊◊
Looking back from more than a half century later, the crash of Pan Am flight 160 was at once a product of its time and a glimpse into the future. It represented an opportunity to learn a wide variety of lessons, some of which were learned to great effect, while others were not, and thus returned to kill again. Some of the causes of the accident might leave a modern reader horrified to discover how things were done in 1973, while others might strike aviation safety experts as surprisingly relevant to the present day. That makes flight 160 both a story of historical interest and a good case study for how human factors, information presentation, and procedural design can turn a hazard into an emergency and an emergency into a fatal accident.
Unfortunately, it was a case study without a happy ending, as the crew navigated their burning airplane to the very threshold of the runway, only to be undone by the consequences of an assumption they had made over half an hour earlier. It was the last assumption in a long string of them, from the checklist that assumed the fire had been put out before opening a window, to the logistics employee who assumed that nitric acid could be cushioned with sawdust because it wasn’t flammable. The outcome was a tragic example of why assumptions are dangerous, and why trust must be paired with verification. Neither flying nor hazmat is inherently safe, and both are as safe as they are today because everyone involved has worked hard to make them so, rather than assuming that everything is fine, or that someone else will take care of it. Because safety will never be someone else’s problem — it always has been and always will be everyone’s problem.
_______________________________________________________________
Note to readers: Because the NTSB report on this crash was unusually vague, my narrative of the accident includes personal deductions about what was meant by certain phrases and concepts and who performed certain actions. I reached best-guess conclusions in many of these areas after consulting with others and examining numerous documents, but my logic is not necessarily unimpeachable. If you know something about this case, or any of the people, companies, airplanes, or systems involved, and you think you can add to or clarify the information in this article, please shoot me an email. Thank you!
_______________________________________________________________
Don’t forget to listen to Controlled Pod Into Terrain, my podcast (with slides!), where I discuss aerospace disasters with my cohosts Ariadne and J! Check out our channel here, and listen to our latest episode about a titanic battle between a BAC 1–11 and some wind. Alternatively, download audio-only versions via RSS.com, or look us up on Spotify!
_______________________________________________________________
Join the discussion of this article on Reddit
Support me on Patreon (Note: I do not earn money from views on Medium!)
Visit r/admiralcloudberg to read and discuss over 260 similar articles
